Analysis of Risk Factors for the Development of Post-Operative Epidural Hematoma after Intracranial Surgery
- Affiliations
-
- 1Department of Neurosurgery, Yeouido St. Mary's Hospital Neuroscience Center, College of Medicine, The Catholic University of Korea, Seoul, Korea. jwi@catholic.ac.kr
- KMID: 1427711
- DOI: http://doi.org/10.13004/kjnt.2012.8.2.79
Abstract
OBJECTIVE
Patients undergoing intracranial operations often suffer from post-operative epidural hematoma (EDH). The incidence and risk factors for with the occurrence of EDH after intracranial operations are not well described previously. The objective of this study was to identify the risk factors and the incidence of post-operative EDH adjacent and regional to the craniotomy.
METHODS
This was a retrospective study of 23 (2.4%) patients, between January 2005 and December 2011, who underwent epidural hematoma evacuation after primary intracranial during this period, 941 intracranial operations were performed. The control group (46 patients) and hematoma group (23 patients) were categorized on the basis of having undergone the same pre-operative diagnosis and treatment within 3 months of their operations. The ages of the hematoma and control group were individually matched to similar ages within 10 years of each other to minimize bias of age.
RESULTS
Univariate analysis showed that the significant pre-operative and intra-operative factors associated with post-operative EDH were a pre-operative Glasgow Coma Scale (GCS) scored <8 (crude odds ratio 8.295), prothrombin ratio >1.0 (p=0.014), prothrombin time (PT) >11.3 sec (p=0.008), intra-operative blood loss >650 mL (p=0.003) and craniotomy size >7,420 mm2 (p=0.023). In multivariate analysis, intra-operative blood loss exceeding 650 mL (median of total patients) placed a patient at significantly increased risk for post-operative EDH.
CONCLUSION
Recognizing the limitations of the study, large intra-operative blood loss, wide craniotomy area, prolonged PT and a pre-operative GCS <8 are presented implicated with an increased risk of post-operative EDH after intracranial surgery.
MeSH Terms
Figure
-

FIGURE 1. Results of computed tomography (CT) examinations. A: CT scan showing intracranial hematoma at right basal ganglia with midline shifting. B: Post-operative immediate brain CT scan showed almost completely removed intracerebral hemorrhage, and also showed large amount of epidural hematoma (EDH) with aggravated mass effect. C: After reoperation was performed to remove the EDH beneath the previous craniectomy site, brain CT scan showed no residual epidural hematoma. A marginal amount of intracerebral hemorrhage remained.
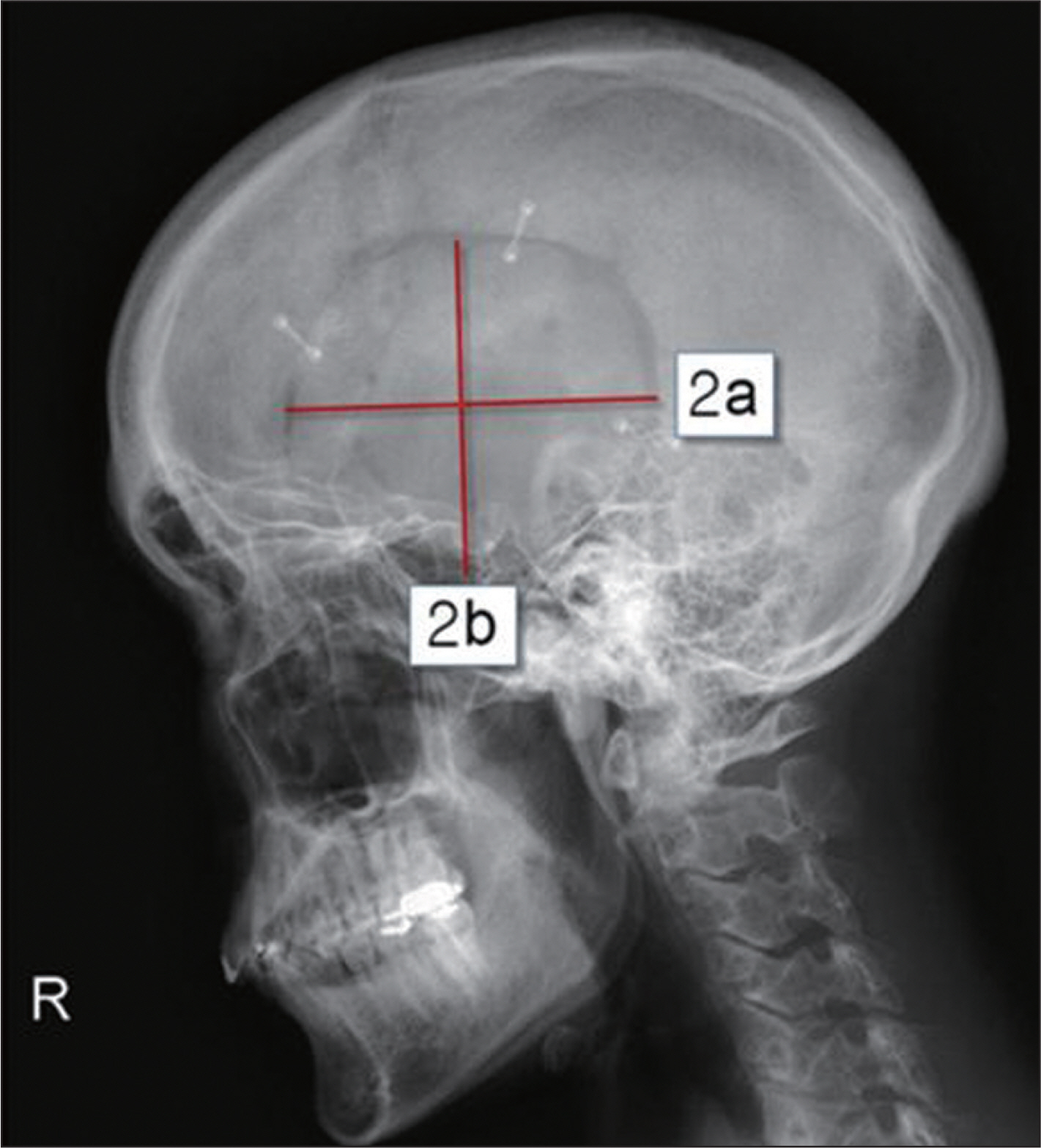
FIGURE 2. Data concerning craniotomy extent. Craniotomy extent was measured from plain lateral skull X-ray that is, from maximal perpendicular diameter (radius a and b) of the craniotomy. The resulting size of craniotomy was then approximated using the formular for a circle (size=π×ab).
Reference
-
1). Altschuler E., Moosa H., Selker RG., Vertosick FT Jr. The risk and efficacy of anticoagulant therapy in the treatment of thromboembolic complications in patients with primary malignant brain tumors. Neurosurgery. 27:74–76. discussion 77. 1990.
Article2). Awad JN., Kebaish KM., Donigan J., Cohen DB., Kostuik JP. Analysis of the risk factors for the development of post-operative spinal epidural haematoma. J Bone Joint Surg Br. 87:1248–1252. 2005.
Article3). Ban SP., Son YJ., Yang HJ., Chung YS., Lee SH., Han DH. Analysis of complications following decompressive craniectomy for traumatic brain injury. J Korean Neurosurg Soc. 48:244–250. 2010.
Article4). Fukamachi A., Koizumi H., Nagaseki Y., Nukui H. Postoperative extradural hematomas: computed tomographic survey of 1105 intracranial operations. Neurosurgery. 19:589–593. 1986.
Article5). Garber ST., Sivakumar W., Schmidt RH. Neurosurgical complications of direct thrombin inhibitors—catastrophic hemorrhage after mild traumatic brain injury in a patient receiving dabigatran. J Neurosurg. 116:1093–1096. 2012.
Article6). Gentleman D., Johnston RA. Postoperative extradural hematoma associated with induced hypertension. Neurosurgery. 17:105–106. 1985.
Article7). Gerlach R., Raabe A., Zimmermann M., Siegemund A., Seifert V. Factor XIII deficiency and postoperative hemorrhage after neurosurgical procedures. Surg Neurol. 54:260–264. discussion 264-265. 2000.
Article8). Guangming Z., Huancong Z., Wenjing Z., Guoqiang C., Xiaosong W. Should epidural drain be recommended after supratentorial craniotomy for epileptic patients? Surg Neurol. 72:138–141. discussion 141. 2009.
Article9). Haft H., Liss H., Mount LA. Massive epidural hemorrhage as a complication of ventricular drainage. J Neurosurg. 17:49–54. 1960.
Article10). Holden MP. Dangers of aspirin before cardiac surgery. BMJ. 305:365–366. 1992.
Article11). Hussain SA., Selway R., Harding C., Polkey CE. The urgent postoperative CT scan: a critical appraisal of its impact. Br J Neurosurg. 15:116–118. 2001.12). Institute SAS. The sas system for windows, version 9.2. Cary, NC: SAS Institute. 1996.13). Jeon JS., Chang IB., Cho BM., Lee HK., Hong SK., Oh SM. Immediate postoperative epidural hematomas adjacent to the craniotomy site. J Korean Neurosurg Soc. 39:335–339. 2006.14). Kalfas IH., Little JR. Postoperative hemorrhage: a survey of 4992 intracranial procedures. Neurosurgery. 23:343–347. 1988.
Article15). Le Roux AA., Nadvi SS. Acute extradural haematoma in the elderly. Br J Neurosurg. 21:16–20. 2007.
Article16). Manian FA., Meyer PL., Setzer J., Senkel D. Surgical site infections associated with methicillin-resistant Staphylococcus aureus: do postoperative factors play a role? Clin Infect Dis. 36:863–868. 2003.17). Palmer JD., Sparrow OC., Iannotti F. Postoperative hematoma: a 5-year survey and identification of avoidable risk factors. Neurosurgery. 35:1061–1064. discussion 1064-1065. 1994.18). Park JE., Kim SH., Yoon SH., Cho KG., Kim SH. Risk factors predicting unfavorable neurological outcome during the early period after traumatic brain injury. J Korean Neurosurg Soc. 45:90–95. 2009.
Article19). Rapanà A., Lamaida E., Pizza V. Multiple postoperative intracerebral haematomas remote from the site of craniotomy. Br J Neurosurg. 12:364–368. 1998.20). Sinar EJ., Lindsay KW. Distant extradural haematoma complicating removal of frontal tumours. J Neurol Neurosurg Psychiatry. 49:442–444. 1986.
Article21). Soff GA. A new generation of oral direct anticoagulants. Arterioscler Thromb Vasc Biol. 32:569–574. 2012.
Article22). Sokolowski MJ., Garvey TA., Perl J 2nd., Sokolowski MS., Cho W., Mehbod AA, et al. Prospective study of postoperative lumbar epidural hematoma: incidence and risk factors. Spine (Phila Pa 1976). 33:108–113. 2008.23). Thiagarajah S. Postoperative care of neurosurgical patients. Int Anesthesiol Clin. 21:139–156. 1983.
Article24). Troupp H. Extradural hematoma during craniotomy. Report of five cases. J Neurosurg. 40:783–785. 1974.25). Yacubian EM., de Andrade MM., Jorge CL., Valério RM. Cerebellar hemorrhage after supratentorial surgery for treatment of epilepsy: report of three cases. Neurosurgery. 45:159–162. 1999.
Article26). Yoshino Y., Aoki N., Oikawa A., Ohno K. Acute epidural hematoma developing during twist-drill craniostomy: a complication of percutaneous subdural tapping for the treatment of chronic subdural hematoma. Surg Neurol. 53:601–604. 2000.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Spontaneous Lumbar Spinal Epidural Hematoma without Rist Factors: A Case Report
- Spontaneous intracranial epidural hematoma following aortic valve replacement: A case report
- Epidural Hematoma after Epidural Catheterization without Coagulopathy: A case report
- Unintended Complication of Intracranial Subdural Hematoma after Percutaneous Epidural Neuroplasty
- Drainage of an acute spinal epidural hematoma that developed without risk factors in the thoracic spine using epidural needle: A case report
