Clinical and Radiological Analysis of Cervical Arthroplasty Compared to Anterior Cervical Discectomy and Fusion in Cervical Disc Disease
- Affiliations
-
- 1Department of Neurological Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. swroh@amc.seoul.kr
- KMID: 1427363
- DOI: http://doi.org/10.13004/jknts.2009.5.2.83
Abstract
OBJECTIVE
Although anterior cervical discectomy and fusion (ACDF) is the most common treatment for degenerative cervical disc disease, concerns about adjacent level degeneration and loss of motion have led to suggestions that total disc replacement may be a better alternative.
METHODS
Since April 2006, 35 cases of cervical arthroplasty have been performed at our institute. Here we compare clinical and radiological results in patients who have cervical disc herniations treated with arthroplasty or with ACDF. We evaluated 67 patients treated for cervical disc herniations with radiculopathy and neck pain, of whom 35 underwent cervical arthroplasty using the Mobi-C(R) (LDR medical, Troyes, France) implant and 32 underwent ACDF using the Solis(R) cage (Stryker Spine, Allendale, NJ). Clinical measurements of outcome included the numeric rating scale (NRS) score for radiculopathy and neck pain, neck disability index (NDI) score, duration of hospital stay and convalescence time. All patients were assessed radiologically by measuring overall cervical lordosis (Cobb's angle), segmental lordosis and segmental range-of-movement (ROM) of operated disc levels and adjacent disc levels.
RESULTS
Mean hospital stay (5.52 vs. 6.26 days, p<0.05) and interval between surgery and return to work (1.15 vs. 2.92 months, p<0.05) were significantly shorter in the arthroplasty than in the ACDF group. After 12 months, mean NDI and neck and extremity NRS scores had improved in both groups. Patients in the arthroplasty group, but not in the ACDF group, maintained their baseline overall preoperative cervical and segmental lordosis scores after surgery. Segmental ROM of adjacent levels were higher in the ACDF group than in the arthroplasty group, and segmental motion of operated level scores in the arthroplasty group were maintained at the last follow-up assessment. The ROM of adjacent segment were smaller in the arthroplasty group than in the ACDF group, but the difference was not statistically significant (p>0.05). In addition, segmental motion of operated level in the arthroplasty group were maintained at the last follow-up assessment. In two cases of arthroplasty group, new bony growth at the treated level, indicating heterotrophic ossification, was suspected based on radiographic (film) results.
CONCLUSION
Although clinical results were similar in the two groups, postoperative recovery was significantly shorter in the arthroplasty group. Postoperative overall cervical and segmental lordosis were reduced in the ACDF group compared with preoperative levels, but not in the arthroplasty group.
MeSH Terms
Figure
-

FIGURE 1 A: Neck disability index (NDI) scores in the arthroplasty and fusion groups (p>0.05). The scores of both groups decreased gradually; however, the greatest decrease was seen in the immediate postoperative period. B: NRS scores of radiculopathy in the arthroplasty and fusion groups (p>0.05). The scores of both groups decreased gradually, but the decreases were greatest in the immediate postoperative period. NRS: nume ical rating scale, VAS: visual analogue scale.
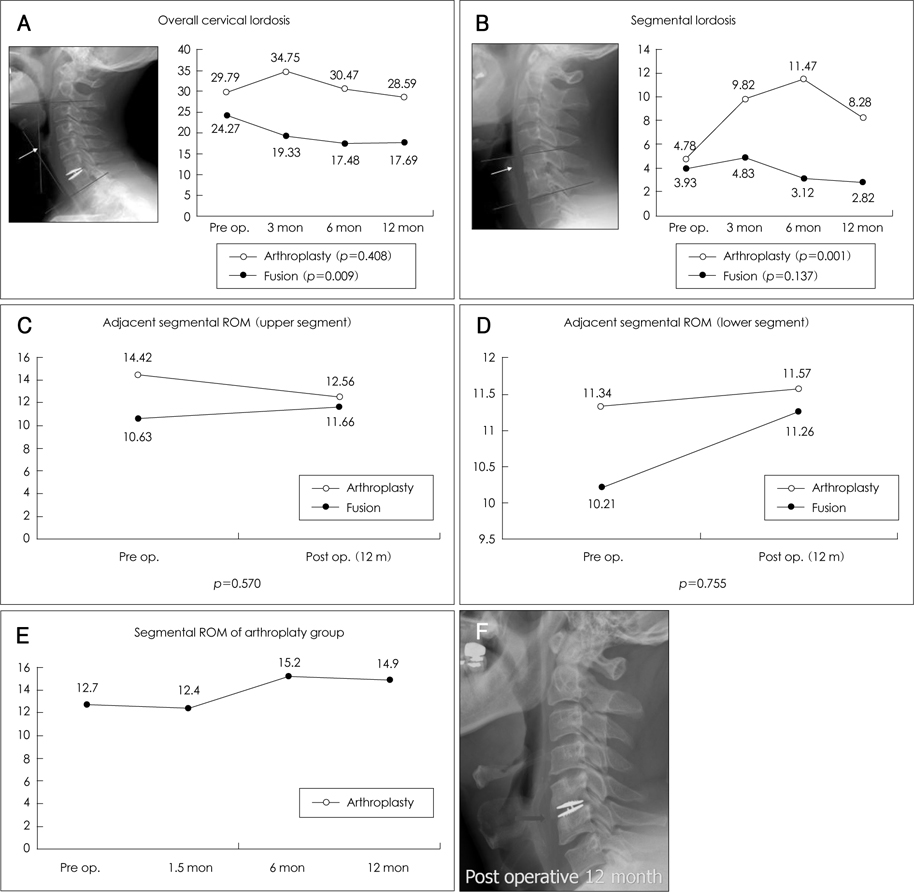
FIGURE 2 A: Overall cervical lordosis in the arthroplasty and fusion groups. Measurement was performed as shown in the left panel. In the arthroplasty group, cervical lordosis increased immediately after surgery, then decreased to preoperative levels. Cervical lordosis in the fusion group gradually decreased after surgery and did not return to preoperative levels. B: Segmental lordosis in the arthroplasty and fusion groups. Measurement was performed as shown in the left panel. In the arthroplasty group, segmental lordosis score increased immediately after surgery, but then decreased after 6 months and returned to preoperative levels. In the fusion group, however, segmental lordosis increased immediately after surgery, then decreased but did not return to preoperative levels. C: Adjacent ROM of the upper level in the arthroplasty and fusion groups. After surgery, upper ROM decreased in the arthroplasty group but increased in the fusion group (p>0.05). D: Adjacent ROM of the lower level in the arthroplasty and fusion groups. After surgery, lower ROM increased in both groups, but the increase was greater in the fusion group (p>0.05). E: Segmental ROM in the arthroplasty group decreased immediately after surgery before increasing to a level greater than the preoperative level. F: In two cases of arthroplasty group, new bony growth at the treated level, indicating heterotrophic ossification, was suspected based on postoperative X-ray. ROM: range of movement.
Reference
-
1. Cummins BH, Robertson JT, Gill SS. Surgical experience with an implanted artificial cervical joint. J Neurosurg. 1998; 88:943–948.
Article2. Eck JC, Humphreys SC, Lim TH, Jeong ST, Kim JG, Hodges SD, et al. Biomechanical study on the effect of cervical spine fusion on adjacent-level intradiscal pressure and segmental motion. Spine (Phila Pa 1976). 2002; 27:2431–2434.
Article3. Goffin J, Geusens E, Vantomme N, Quintens E, Waerzeggers Y, Depreitere B, et al. Long-term follow-up after interbody fusion of the cervical spine. J Spinal Disord Tech. 2004; 17:79–85.
Article4. Hilibrand AS, Carlson GD, Palumbo MA, Jones PK, Bohlman HH. Radiculopathy and myelopathy at segments adjacent to the site of a previous anterior cervical arthrodesis. J Bone Joint Surg Am. 1999; 81:519–528.
Article5. Katsuura A, Hukuda S, Saruhashi Y, Mori K. Kyphotic malalignment after anterior cervical fusion is one of the factors promoting the degenerative process in adjacent intervertebral levels. Eur Spine J. 2001; 10:320–324.
Article6. Kim SH, Shin HC, Shin DA, Kim KN, Yoon do H. Early clinical experience with the mobi-C disc prosthesis. Yonsei Med J. 2007; 48:457–464.
Article7. Kim SW, Limson MA, Kim SB, Arbatin JJ, Chang KY, Park MS, et al. Comparison of radiographic changes after ACDF versus Bryan disc arthroplasty in single and bi-level cases. Eur Spine J. 2009; 18:218–231.
Article8. Kim SW, Shin JH, Arbatin JJ, Park MS, Chung YK, McAfee PC. Effects of a cervical disc prosthesis on maintaining sagittal alignment of the functional spinal unit and overall sagittal balance of the cervical spine. Eur Spine J. 2008; 17:20–29.
Article9. Kulkarni V, Rajshekhar V, Raghuram L. Accelerated spondylotic changes adjacent to the fused segment following central cervical corpectomy: magnetic resonance imaging study evidence. J Neurosurg. 2004; 100:1 Suppl Spine. 2–6.
Article10. Mummaneni PV, Burkus JK, Haid RW, Traynelis VC, Zdeblick TA. Clinical and radiographic analysis of cervical disc arthroplasty compared with allograft fusion: a randomized controlled clinical trial. J Neurosurg Spine. 2007; 6:198–209.
Article11. Nabhan A, Ahlhelm F, Pitzen T, Steudel WI, Jung J, Shariat K, et al. Disc replacement using Pro-Disc C versus fusion: a prospective randomised and controlled radiographic and clinical study. Eur Spine J. 2007; 16:423–430.
Article12. Pickett GE, Rouleau JP, Duggal N. Kinematic analysis of the cervical spine following implantation of an artificial cervical disc. Spine (Phila Pa 1976). 2005; 30:1949–1954.
Article13. Sasso RC, Best NM, Metcalf NH, Anderson PA. Motion analysis of bryan cervical disc arthroplasty versus anterior discectomy and fusion: results from a prospective, randomized, multicenter, clinical trial. J Spinal Disord Tech. 2008; 21:393–399.
Article14. Sasso RC, Smucker JD, Hacker RJ, Heller JG. Artificial disc versus fusion: a prospective, randomized study with 2-year follow-up on 99 patients. Spine (Phila Pa 1976). 2007; 32:2933–2942.15. Shim CS, Lee SH, Park HJ, Kang HS, Hwang JH. Early clinical and radiologic outcomes of cervical arthroplasty with Bryan Cervical Disc prosthesis. J Spinal Disord Tech. 2006; 19:465–470.
Article16. Silber JS, Anderson DG, Daffner SD, Brislin BT, Leland JM, Hilibrand AS, et al. Donor site morbidity after anterior iliac crest bone harvest for single-level anterior cervical discectomy and fusion. Spine (Phila Pa 1976). 2003; 28:134–139.
Article17. St John TA, Vaccaro AR, Sah AP, Schaefer M, Berta SC, Albert T, et al. Physical and monetary costs associated with autogenous bone graft harvesting. Am J Orthop. 2003; 32:18–23.18. van Jonbergen HP, Spruit M, Anderson PG, Pavlov PW. Anterior cervical interbody fusion with a titanium box cage: early radiological assessment of fusion and subsidence. Spine J. 2005; 5:645–649.
Article19. Weinhoffer SL, Guyer RD, Herbert M, Griffith SL. Intradiscal pressure measurements above an instrumented fusion. A cadaveric study. Spine (Phila Pa 1976). 1995; 20:526–531.20. Wenger M, Hoonacker P, Zachee B, Lange R, Markwalder TM. Bryan cervical disc prostheses: preservation of function over time. J Clin Neurosci. 2009; 16:220–225.
Article21. Yoon DH, Yi S, Shin HC, Kim KN, Kim SH. Clinical and radiological results following cervical arthroplasty. Acta Neurochir (Wien). 2006; 148:943–950.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Total Cervical Disc Replacement using Artificial Disc in Cervical Disc Herniations
- Anterior Cervical Discectomy
- A Comparison of Anterior Cervical Discectomy and Fusion versus Fusion Combined with Artificial Disc Replacement for Treating 3-Level Cervical Spondylotic Disease
- Results of Anterior Cervical Discectomy without Interbody Fusion
- Analysis of Noninstrumented Anterior Cervical Discectomy and Interbody Fusion in Degenerative Cervical Disease
