Korean J Urol.
2008 Nov;49(11):1041-1045. 10.4111/kju.2008.49.11.1041.
Voiding and Sexual Dysfunction following Total Mesorectal Excision and Autonomic Nerve Preservation for Rectal Cancer in Males:A Prospective Study
- Affiliations
-
- 1Department of Urology, Korea Cancer Center Hospital, Seoul, Korea. urodori@yahoo.co.kr
- 2Department of Surgery, Korea Cancer Center Hospital, Seoul, Korea.
- KMID: 1328179
- DOI: http://doi.org/10.4111/kju.2008.49.11.1041
Abstract
-
PURPOSE: We designed a prospective study to evaluate the effects of total mesorectal excision and autonomic nerve preservation(TME-ANP) on postoperative genitourinary function in the course of time and the quantitative effects of various peri-operative risk factors on the postoperative genitourinary dysfunction.
MATERIALS AND METHODS
Forty-five patients who underwent TME-ANP with rectal cancer were prospectively examined before and after operation, as well after the first, third and sixth postoperative month. The preoperative urological evaluation consisted of International Prostate Symptom Score(IPSS), Erectile Function Domain score in International Index of Erectile Function(IIEF-EFD), Ejaculation domain in Male Sexual Health Questionnaire(MSHQ-EjD) and urodynamic study.
RESULTS
Preoperative IPSS decreased significantly in postoperative 1 month. But there was no difference between preoperative IPSS and postoperative IPSS after 3 month of operation. Erectile function significantly decreased in the course of time(p-trend<0.05). Ejaculation function also significantly decreased after 1 month of operation, however no significant change of MSHQ-EjD was observed thereafter. Multivariate analysis revealed history of abdominoperineal resection and baseline mild erectile dysfunction were found to be the risk factors of decreasing erectile function. Diabetes was associated with diminishing ejaculatory function.
CONCLUSIONS
While the voiding dysfuncion was no longer problematic following TME-ANP, substantial number of sexual dysfunction persisted despite TME-ANP.
Keyword
MeSH Terms
Figure
-

Fig. 1. Study design. UDS: urodynamic study, TRUS: transrectal ultrasonography.

Fig. 2. International Prostate Symptom Score (IPSS) change before and after rectal cancer operation. ∗: p<0.05 compared to preoperation.
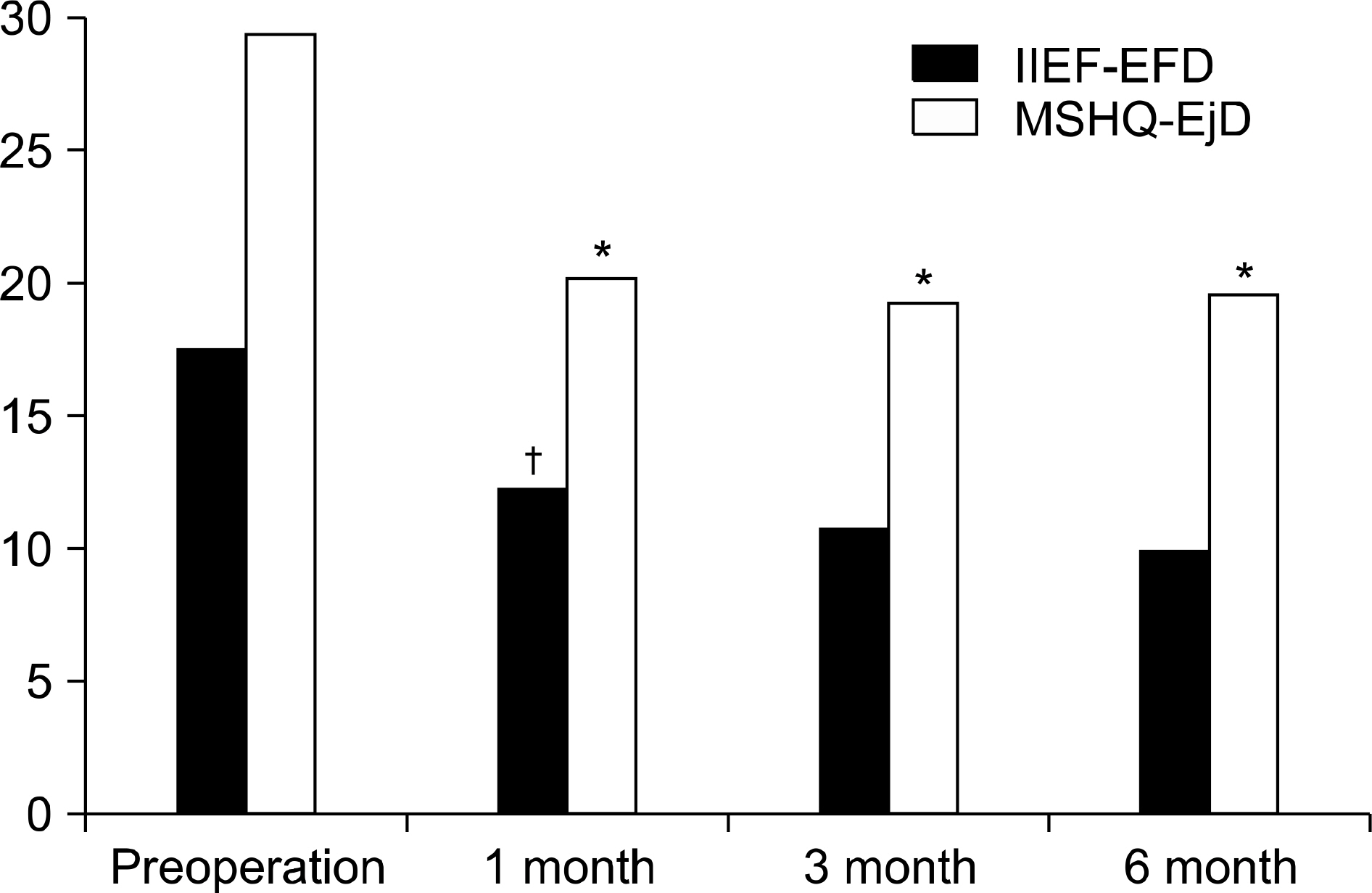
Fig. 3. Erectile Function Domain score in International Index of Erectile Function (IIEF-EFD) and Ejaculation score in Male Sexual Health Questionnaire (MSHQ-EjD) changes of before and after rectal cancer operation. ∗: p<0.05 compared to preoperation, †: significant decline of IIEF-EFD in the course of time.
Reference
-
References
1. Paick JS, Oh SJ, Park JG, Choe KJ, Kim SH. Change in potency following rectal cancer surgery. Korean J Urol. 1994; 35:655–64.2. Lee SE, Oh SJ, Lee MS, Seo JM, Park JG, Choi KJ, et al. Voiding dysfunction after rectal cancer surgery: analysis by symptom score and residual urine volume. Korean J Urol. 1994; 35:156–64.3. Oh SJ, Park JG, Choe KJ, Lee SE. Bladder dysfunction after rectal cancer surgery: urodynamic evaluation. Korean J Urol. 1993; 34:689–704.4. Havenga K, Maas CP, DeRuiter MC, Welvaart K, Trimbos JB. Avoiding longterm disturbance to bladder and sexual dysfunction in pelvic surgery, particularly with rectal cancer. Semin Surg Oncol. 2000; 18:235–43.5. Leveckis J, Boucher NR, Parys BT, Reed MW, Shorthouse AJ, Anderson JB. Bladder and erectile dysfunction before and after rectal surgery for cancer. Br J Urol. 1995; 76:752–6.
Article6. Vironen JH, Kairaluoma M, Aalto AM, Kellokumpu IH. Impact of functional results on quality of life after rectal cancer surgery. Dis Colon Rectum. 2006; 49:568–78.
Article7. Engel J, Kerr J, Schlesinger-Raab A, Eckel R, Sauer H, Holzel D. Quality of life in rectal cancer patients: a four-year prospective study. Ann Surg. 2003; 238:203–13.8. Camilleri-Brennan J, Steele RJ. Prospective analysis of quality of life and survival following mesorectal excision for rectal cancer. Br J Surg. 2001; 88:1617–22.
Article9. Heald RJ. Total mesorectal excision is optimal surgery for rectal cancer: a Scandinavian consensus. Br J Surg. 1995; 82:1297–9.
Article10. Heald RJ. The holy plane of rectal surgery. J R Soc Med. 1988; 81:503–8.
Article11. Sugihara K, Moriya Y, Akasu T, Fujita S. Pelvic autonomic nerve preservation for patients with rectal carcinoma. Oncologic and functional outcome. Cancer. 1996; 78:1871–80.
Article12. Mundy AR. An anatomical explanation for bladder dysfunction following rectal and uterine surgery. Br J Urol. 1982; 54:501–4.
Article13. Zinreich ES, Derogatis LR, Herpst J, Auvil G, Piantadosi S, Order SE. Pre and posttreatment evaluation of sexual function in patients with adenocarcinoma of the prostate. Int J Radiat Oncol Biol Phys. 1990; 19:729–32.
Article14. Kim NK. Anatomic basis of sharp pelvic dissection for curative resection of rectal cancer. Yonsei Med J. 2005; 46:737–49.
Article15. Nesbakken A, Nygaard K, Bull-Njaa T, Carlsen E, Eri LM. Bladder and sexual dysfunction after mesorectal excision for rectal cancer. Br J Surg. 2000; 87:206–10.
Article16. Havenga K, Enker WE, McDermott C, Cohen AM, Minsky BD, Guillem J. Male and female sexual and urinary function after total mesorectal excision with autonomic nerve preservation for carcinoma of the rectum. J Am Coll Surg. 1996; 182:495–502.17. Masui H, Ike H, Yamaguchi S, Oki S, Shimada H. Male sexual function after autonomic nerve-preserving operation for rectal cancer. Dis Colon Rectum. 1996; 39:1140–5.
Article18. Kim NK, Aahn TW, Park JK, Lee KY, Lee WH, Sohn SK, et al. Assessment of sexual and voiding function after total mesorectal excision with pelvic autonomic nerve preservation in males with rectal cancer. Dis Colon Rectum. 2002; 45:1178–85.
Article19. Sterk P, Shekarriz B, Gunter S, Nolde J, Keller R, Bruch HP, et al. Voiding and sexual dysfunction after deep rectal resection and total mesorectal excision: prospective study on 52 patients. Int J Colorectal Dis. 2005; 20:423–7.20. Moreland RB. Is there a role of hypoxemia in penile fibrosis; a viewpoint presented to the Society for the Study of Impotence. Int J Impot Res. 1998; 10:113–20.
Article21. Bahnson RR, Catalona WJ. Papaverine testing of impotent patients following nerve-sparing radical prostatectomy. J Urol. 1988; 139:773–4.
Article22. Jannini EA, Screponi E, Carosa E, Pepe M, Lo Giudice F, Trimarchi F, et al. Lack of sexual activity from erectile dysfunction is associated with a reversible reduction in serum testosterone. Int J Androl. 1999; 22:385–92.
Article23. Schmidt CE, Bestmann B, Kuchler T, Kremer B. Factors influencing sexual function in patients with rectal cancer. Int J Impot Res. 2005; 17:231–8.
Article24. Rabbani F, Stapleton AM, Kattan MW, Wheeler TM, Scardino PT. Factors predicting recovery of erections after radical prostatectomy. J Urol. 2000; 164:1929–34.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Anatomic Basis of Sharp Pelvic Dissection for Curative Resection of Rectal Cancer
- Anatomic Basis of Sharp Pelvic Dissection for Total Mesorectal Excision with Pelvic Autonomic Nerve Preservation for Rectal Cancer
- Assessment of Sexual and Voiding Function after Total Mesorectal Excision with Pelvic Autonomic Nerve Preservation in Male Rectal Cancer Patients
- Effectiveness of Partial Autonomic Nerve Preservation Surgery for Sexual Function in the Male in the Advanced Rectal Cancers
- Rectal Cancer: Function-preserving Surgery
