Korean J Ophthalmol.
2004 Jun;18(1):79-83. 10.3341/kjo.2004.18.1.79.
An Atypical Case of Aicardi Syndrome with Favorable Outcome
- Affiliations
-
- 1Department of Ophthalmology, Dongguk University College of Medicine, Kyongju, Korea.
- 2Department of Pediatrics, Dongguk University College of Medicine, Kyongju, Korea.
- KMID: 1115788
- DOI: http://doi.org/10.3341/kjo.2004.18.1.79
Abstract
- Aicardi syndrome is a severe congenital disorder characterized by infantile spasms, chorioretinal lacunae, and agenesis or hypogenesis of the corpus callosum. A 6 month old female had developed abnormal eye movement and seizures of the complex partial type and myoclonic type. MRI pictures of the patient revealed the presence of genu associated with agenesis of the rest of corpus callosum. A funduscopic examination revealed bilateral small, solitary, pale areas with sharp borders, some of which had minimal surrounding pigmentation (chorioretinal lacunae), especially clustered around the disc, and they were more prominent on the left side. We report here on the unusual findings of a complex partial seizure, myoclonic seizure and the atypical EEG finding in addition to the well-known characteristic clinical and imaging findings of a patient with Aicardi syndrome.
MeSH Terms
-
Anticonvulsants/therapeutic use
Arachnoid Cysts/*pathology
Corpus Callosum/*abnormalities
Electroencephalography
Epilepsies, Myoclonic/drug therapy/*pathology
Epilepsies, Partial/drug therapy/*pathology
Female
Humans
Infant
Magnetic Resonance Imaging
Retinal Diseases/*pathology
Spasms, Infantile/drug therapy/*pathology
Syndrome
Figure
-
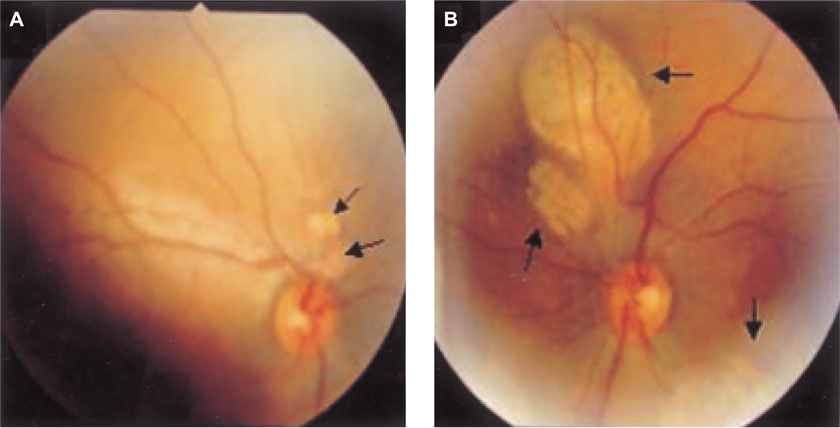
Fig. 1 Bilateral variable size, discrete, pale areas with sharp borders, some of which had a minimal surrounding pigmentation. (Chorioretinal lacunae, black arrow). They are especially clustered around the disc, and they are more prominent on the left eye. (Right eye (A), Left eye(B))

Fig. 2 A sagittal midline T1-weighted MR image shows hypogenesis of the corpus callosum (black arrow). The genu of corpus callosum can be observed. (white arrow).

Fig. 3 An axial T2-weighted MR imaged show a large multi-lobulated midline cystic mass, that is lodged at the interhemispheric area. There are bands of right subependymal gray matter heterotopia. (white arrow)
Reference
-
1. Aicardi J, Lefebrve J, Lerique-Koechlin A. A new syndrome: spasm in flexion, callosal agenesis, ocular abnormalities. Electroencephalogr Clin Neurophysiol. 1965. 9:609–610.2. Aicardi J, Chevrie JJ, Rousselie F. Le syndrome spasmes en flexion, agenesic calleuse, anomalies chorio-retiniennes. Arch Franc Pediatr. 1969. 26:1103–1120.3. Ballabio A, Andria G. Deletions and translocations involving the distal short arm of the human X chromosome: review and hypotheses. Hum Mol Genet. 1992. 1:221–227.4. Ropers HH, Zuffardi O, Bianchi E, Tiepolo L. Agenesis of corpus callosum, ocular, and skeletal anomalies (X-linked dominant Aicardi's syndrome) in a girl with balanced X/3 translocation. Hum Genet. 1982. 61:364–368.5. Smith CD, Ryan SJ, Hoover SL, Baumann RJ. Magnetic resonance imaging of the brain in Aicardi's syndrome. Report of 20 patients. J Neuroimaging. 1996. 6:214–221.6. Moom JL, Jung KH, Kang SY. Aicardi syndrome. J Korean Rehab Soc. 1999. 24:576–581.7. Yang IS, You KO, Chae SA, Kim DH, Park JY, Kang IW. A case of Aicardi syndrome with cleft lip and palate. J Korean Pediatr Soc. 1993. 36:1325–1230.8. Park BR, Jung HJ, Go CJ, Sed YS. A case of Aicardi's syndrome. J Korean Pediatr Soc. 1982. 12:1285–1288.9. Kim SW, Lee EK, Lee KH. A case of Aicardi's syndrome. J Korean Ophthalmol Soc. 1997. 38:511–515.10. Carney SH, Brodsky MC, Good WV, Glasier CM, Greibel ML, Cunniff C. Aicardi syndrome: more than meets the eye. Surv Ophthalmol. 1993. 37:419–424.11. Gloor P, Pulido JS, Judisch GF. Magnetic resonance imaging and fundus findings in a patient with Aicardi's syndrome. Arch Ophthalmol. 1989. 107:922–923.12. Goldberg MF. Persistent fetal vasculature (PFV): an integrated interpretation of signs and symptoms associated with persistent hyperplastic primary vitreous (PHPV). Am J Ophthalmol. 1997. 124:587–626.13. Chiu NC, Shen EY, Fang SR. Aicardi's syndrome in a female infant with a family history of miscarried smale sibling. J Formos Med Assoc. 1992. 91:624–626.14. Hoyt CS, Billson F, Ouvrier R, Wise G. Ocular features of Aicardi's syndrome. Arch Ophthalmol. 1978. 96:291–295.15. Taylor DS. The genetic implications of optic disc anomalies. Trans Ophthalmol Soc UK. 1985. 104:853–866.16. Beby F, Zech C, Touraine R, Guibaud R, Masset H, Trepsat C, Denis P. Persistent hyperplastic primary vitreous syndrome in a girl with Aicardi syndrome. J Fr Ophtalmol. 2000. 23:703–707.17. Cruz-Velarde JA, Garzo C, Garcia-Munoz S, Gil R, Munoz L. Clinical and prognostic heterogeneity in Aicardi's syndrome: a description of two cases. Rev Neurol. 1999. 28:784–785.18. Neidich JA, Nussbaum RL, Packer RJ, Emanuel BS, Puck JM. Heterogeneity of clinical severity and molecular lesions in Aicardi syndrome. J Pediatr. 1990. 116:911–917.19. Htsuka Y, Oka E, Terasaki T, Ohtahara S. Aicardi syndrome:a longitudinal clinical and electroencephalographic study. Epilepsia. 1993. 34:627–634.20. Yacoub M, Missaoui N, Tabarli B, Ghorbel M, Tlili K, Selmi H, Essoussi A. Aicardi syndrome with favorable outcome. Arch Pediatr. 2003. 10:530–532.
