Peripheral Anterior Synechiae and Ultrasound Biomicroscopic Parameters in Angle-Closure Glaucoma Suspects
- Affiliations
-
- 1Department of Ophthalmology, Korea University College of Medicine, Seoul, Korea. yongykim@mail.korea.ac.kr
- 2Kong Eye Center, Seoul, Korea.
- KMID: 1101913
- DOI: http://doi.org/10.3341/kjo.2007.21.2.106
Abstract
- PURPOSE: To investigate the correlation between peripheral anterior synechia (PAS) and the quantitative anterior chamber angle parameters measured by ultrasound microscopy (UBM) in angle-closure glaucoma suspect (ACGS) eyes. METHODS: Eyes were defined ACGS as having occludable angles and intraocular pressure less than 21 mm Hg without glaucomatous optic nerve head. The gonioscopic criteria for ACGS were the trabecular meshwork invisible in 3 or more quadrants of the entire angle and the angular width less than 20 degrees by Shaffer classification. Twenty-seven eyes of 20 patients underwent anterior chamber angle and ciliary body imaging with UBM. Angle opening distance (AOD500), angle recess area (ARA), trabecular-ciliary process distance (TCPD) and trabecular-iris angle (TIA) were measured from the UBM images at each quadrant. RESULTS: The AOD500, ARA, and TIA were not significantly different between the eyes with PAS (9 eyes) and without PAS (18 eyes) at each quadrant. However, the TCPD was significantly shorter in the superior quadrant when compared with the eyes without PAS (mean: 405.3+/-70.9 micrometer vs 536.4+/-140.5 micrometer) (p<0.05). CONCLUSIONS: The results suggest that the shorter distance from trabecular meshwork to ciliary body or the anterior placement of ciliary process may play a role in the development of PAS in ACGS eyes.
Keyword
MeSH Terms
-
Aged
Anterior Chamber/*ultrasonography
Ciliary Body/pathology/ultrasonography
Cross-Sectional Studies
Female
Follow-Up Studies
Glaucoma, Angle-Closure/pathology/*ultrasonography
Gonioscopy
Humans
Male
Microscopy, Acoustic/*methods
Middle Aged
Prognosis
Retrospective Studies
Severity of Illness Index
Trabecular Meshwork/pathology/ultrasonography
Figure
-
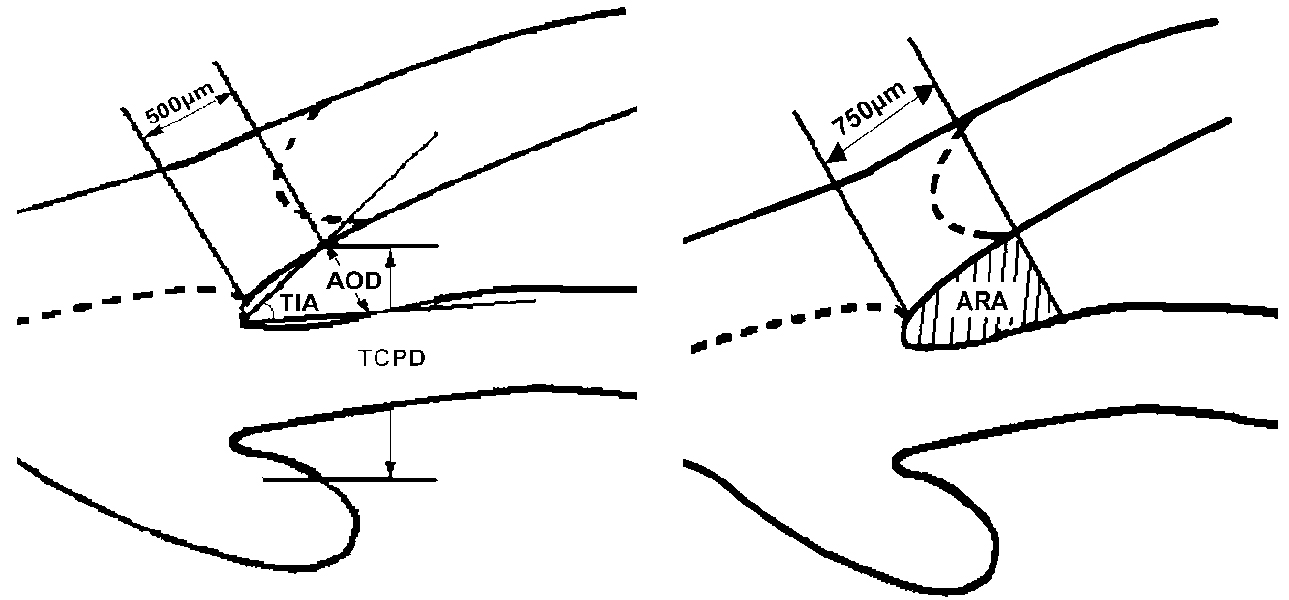
Fig. 1 Schematic representation of UBM anterior chamber angle measurement. Angle opening distance (AOD500) is defined as the length of the line drawn from the point on the corneal endothelial surface 500 µm anterior to the scleral spur to the iris surface perpendicular to the corneal endothelial surface. Trabecular-iris angle (TIA) is defined as an angle formed with the apex at the iris recess and the arms passing through the point on the meshwork 500 µm from the scleral spur and the point on the iris perpendicularly opposite. Trabecular ciliary process distance (TCPD) is defined as the distance between a point 500 µm from the scleral spur and the ciliary process on the line that is perpendicular through the iris. Angle recess area (ARA) is defined as the triangular area bordered by the anterior iris surface, corneal endothelium, and a line perpendicular to the corneal endothelium drawn to the iris surface from a point 750 µm anterior to the scleral spur.
Reference
-
1. Inoue T, Yamamoto T, Kitazawa Y. Distribution and morphology of peripheral anterior synechiae in primary angle-closure glaucoma. J Glaucoma. 1993. 3:171–176.2. Kronfeld PC. Delayed restoration of the anterior chamber. Am J Ophthalmol. 1954. 38:453–465.3. Choi JS, Kim YY. Relationship between the extent of peripheral anterior synechiae and the severity of visual field defects in primary angle-closure glaucoma. Korean J Ophthalmol. 2004. 18(2):100–105.4. Aung T, Lim MC, Chan YH, et al. Configuration of the drainage angle, intraocular pressure, and optic disc cupping in subjects with chronic angle-closure glaucoma. Ophthalmology. 2005. 112(1):28–32.5. West RH. Creeping angle-closure glaucoma: the influence of iridotomy and iridectomy. Aust N Z J Ophthalmol. 1992. 20:23–28.6. Yamamoto T, Shirato S. Treatment of primary angle-closure glaucoma by argon laser iridotomy: a long-term follow-up. Jpn J Ophthalmol. 1985. 29:1–12.7. Choi JS, Kim YY. Progression of peripheral anterior synechiae after laser iridotomy. Am J Ophthalmol. 2005. 140:1125–1127.8. Kim YY, Jung HR. Clarifying the nomenclature for primary angle-closure glaucoma. Surv Ophthalmol. 1997. 42:125–136.9. Pavlin CJ, Ritch R, Foster FS. Ultrasound biomicroscopy in plateau iris syndrome. Am J Ophthalmol. 1992. 113:390–395.10. Pavlin CJ, Foster FS. Ultrasound Biomicroscopy of the Eye. 1995. New York: Springer-Verlag;140–154.11. Pavlin CJ, Harasiewicz K, Eng P, et al. Ultrasound biomicroscopy of anterior segment structures in normal and glaucomatous eyes. Am J Ophthalmol. 1992. 113:381–389.12. Gorin G. Shortening of the angle of the anterior chamber in angle closure glaucoma. Am J Ophthalmol. 1960. 49:141–146.13. Lowe RF. Clinical types of primary angle closure glaucoma. Aust NZ J Ophthalmol. 1988. 16:245–250.14. Lowe RF. Aetiology of the anatomical basis for primary angle closure glaucoma. Br J Ophthalmol. 1970. 54:161–169.15. Sakuma T, Sawada A, Yamamoto T, et al. Appositional angle closure in eyes with narrow angles: an ultrasound biomicroscopic study. J Glaucoma. 1997. 6:165–169.16. Phillips CI. Sectorial distribution of goniosynechiae. Br J Ophthalmol. 1956. 40:129–135.17. Phillips CI. Closed-angle glaucoma: significance of sectorial variations in angle depth. Br J Ophthalmol. 1956. 40:136–143.18. Bhargava SK, Leighton DA, Phillips CI. Early angle-closure glaucoma. Distribution of iridotrabecular contact and response to pilocarpine. Arch Ophthalmol. 1973. 89:369–372.19. Barkan O. Etiology of narrow-angle glaucoma; report of a case of glaucoma secondary to anterior displacement of the lens iris diaphragm. Am J Ophthalmol. 1953. 36:901–906.20. Barkan O. Narrow-angle glaucoma; effect of miosis on the narrow-angle mechanism and intraocular pressure. Am J Ophthalmol. 1953. 36:1387–1388.21. Kunimatsu S, Tomidokoro A, Mishima K, et al. Prevalence of appositional angle closure determined by ultrasonic biomicroscopy in eyes with shallow anterior chambers. Ophthalmology. 2005. 112:407–412.22. Salmon JF. Predisposing factors for chronic angle-closure glaucoma. Prog Retin Eye Res. 1998. 18:121–132.23. Yeung BY, Ng PW, Chiu TY, et al. Prevalence and mechanism of appositional angle closure in acute primary angle closure after iridotomy. Clinical and Experimental Ophthalmology. 2005. 33:478–482.24. Ritch R. Plateau iris is caused by abnormally positioned ciliary processes. J Glaucoma. 1992. 1:23–26.25. Leighton DA, Phillips CI, Tsukahara S. Profile of presenting states of eyes in angle-closure glaucoma. Br J Ophthalmol. 1970. 55:577–584.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Effect of YAG Laser Iridotomy on IOP in Chronic Angle-closure Glaucoma
- Glaucoma in Leprosy
- Relationship between the Extent of Peripheral Anterior Synechiae and the Severity of Visual Field Defects in Primary Angle-closure Glaucoma
- Clinical Factors that Influence Intraocular Pressure Change after Cataract Surgery in Primary Open-Angle Glaucoma and Angle-Closure Glaucoma
- Ultrasound biomicroscopic dimensions of the anterior chamber in angle-closure glaucoma patients
