J Korean Med Sci.
2011 Jul;26(7):865-869. 10.3346/jkms.2011.26.7.865.
Usefulness of Quantitative Endotracheal Aspirate Cultures in Intensive Care Unit Patients with Suspected Pneumonia
- Affiliations
-
- 1Division of Pulmonary & Critical Care Medicine, Department of Internal Medicine, Cheongju St. Mary Hospital, Cheongju, Korea.
- 2Division of Pulmonary & Critical Care Medicine, Department of Internal Medicine, University of Ulsan College of Medicine, Asan Medical Center, Seoul, Korea. sbhong@amc.seoul.kr
- 3Department of Laboratory Medicine, University of Ulsan College of Medicine, Asan Medical Center, Seoul, Korea.
- KMID: 1094255
- DOI: http://doi.org/10.3346/jkms.2011.26.7.865
Abstract
- It is difficult to differentiate pathogens responsible for pneumonia or colonization in patients with an endotracheal tube or in patients that have undergone tracheostomy. We evaluated the clinical usefulness of quantitative endotracheal aspirates cultures and sought to determine the result threshold level for positivity. The authors performed this retrospective cohort study between December 1, 2004 and January 31, 2006. Forty-five suspected pneumonia patients admitted to an intensive care unit (ICU) with quantitative bronchoalveolar lavage (BAL) and endotracheal aspirate (EA) culture results were enrolled. Using a threshold of 10(5) cfu/mL, 10 of the 45 (22.2%) quantitative EA cultures were positive, as compared with 7 (15.6%) BAL cultures. When BAL culture findings were used as the reference, the sensitivity and specificity of quantitative EA cultures were 85.7% and 89.5%, respectively, at a threshold of 10(5) cfu/mL, and 85.7% and 94.7%, respectively, at a threshold of 10(6) cfu/mL. Of the 10 EA culture positive patients, 2 patients with a result of -10(5) cfu/mL were BAL culture negative. The quantitative EA culture is a useful non-invasive tool for the diagnosis of pneumonia pathogens. It is suggested that a threshold level of 10(6) cfu/mL is appropriate.
MeSH Terms
Figure
-
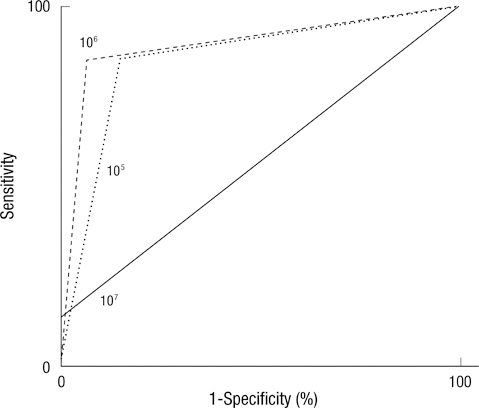
Fig. 1 ROC curve of quantitative EA culture.
Reference
-
1. Baughman RP. Diagnosis of ventilator-associated pneumonia. Microbes Infect. 2005. 7:262–267.2. American Thoracic Society. Infectious Diseases Society of America. Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am J Respir Crit Care Med. 2005. 171:388–416.3. Lambotte O, Timsit JF, Garrouste-Orgeas M, Misset B, Benali A, Carlet J. The significance of distal bronchial samples with commensals in ventilator-associated pneumonia: colonizer or pathogen? Chest. 2002. 122:1389–1399.4. Albert S, Kirchner J, Thomas H, Behne M, Schur J, Brade V. Role of quantitative cultures and microscopic examinations of endotracheal aspirates in the diagnosis of pulmonary infections in ventilated patients. J Hosp Infect. 1997. 37:25–37.5. Tsai SH, Cohen SS, Fenger EP. Bronchial perforation as a complication of bronchoscopy. Am Rev Tuberc. 1958. 78:106–110.6. Prakash UB, Offord KP, Stubbs SE. Bronchoscopy in North America: the ACCP survey. Chest. 1991. 100:1668–1675.7. Jolliet P, Chevrolet JC. Bronchoscopy in the intensive care unit. Intensive Care Med. 1992. 18:160–169.8. Valentine VG, Rizk NW, Hancock EW. A complication during bronchoscopy. Hosp Pract (Off Ed). 1993. 28:22. 27.9. Pereira W, Kovnat DM, Khan MA, Iacovino JR, Spivack ML, Snider GL. Fever and pneumonia after flexible fiberoptic bronchoscopy. Am Rev Respir Dis. 1975. 112:59–64.10. Kiss K, Pápai Z, Szima B, Kis S, Strausz J. Fiberoptic bronchoscopy in intensive care units. Orv Hetil. 1996. 137:1689–1691.11. Hammer DL, Aranda CP, Galati V, Adams FV. Massive intrabronchial aspiration of contents of pulmonary abscess after fiberoptic bronchoscopy. Chest. 1978. 74:306–307.12. Friedman RL. Selective pneumothorax: a complication of bronchoscopy. Dis Chest. 1955. 27:213–215.13. Bergmans DC, Bonten MJ, De Leeuw PW, Stobberingh EE. Reproducibility of quantitative cultures of endotracheal aspirates from mechanically ventilated patients. J Clin Microbiol. 1997. 35:796–798.14. Chastre J, Fagon JY. Ventilator-associated pneumonia. Am J Respir Crit Care Med. 2002. 165:867–903.15. Brun-Buisson C, Fartoukh M, Lechapt E, Honoré S, Zahar JR, Cerf C, Maitre B. Contribution of blinded, protected quantitative specimens to the diagnostic and therapeutic management of ventilator-associated pneumonia. Chest. 2005. 128:533–544.16. Clec'h C, Jauréguy F, Hamza L, Karoubi P, Fosse JP, Hamdi A, Vincent F, Gonzalez F, Cohen Y. Agreement between quantitative cultures of postintubation tracheal aspiration and plugged telescoping catheter, protected specimen brush, or BAL for the diagnosis of nosocomial pneumonia. Chest. 2006. 130:956–961.17. Cook D, Mandell L. Endotracheal aspiration in the diagnosis of ventilator-associated pneumonia. Chest. 2000. 117:4 Suppl 2. 195S–197S.18. Elatrous S, Boukef R, Ouanes Besbes L, Marghli S, Nooman S, Nouira S, Abroug F. Diagnosis of ventilator-associated pneumonia: agreement between quantitative cultures of endotracheal aspiration and plugged telescoping catheter. Intensive Care Med. 2004. 30:853–858.19. Fangio P, Rouquette-Vincenti I, Rousseau JM, Soullié B, Brinquin L. Diagnosis of ventilator-associated pneumonia: a prospective comparison of the telescoping plugged catheter with the endotracheal aspirate. Ann Fr Anesth Reanim. 2002. 21:184–192.20. Fujitani S, Yu VL. Diagnosis of ventilator-associated pneumonia: focus on nonbronchoscopic techniques (nonbronchoscopic bronchoalveolar lavage, including mini-BAL, blinded protected specimen brush, and blinded bronchial sampling) and endotracheal aspirates. J Intensive Care Med. 2006. 21:17–21.21. Papazian L, Thomas P, Garbe L, Guignon I, Thirion X, Charrel J, Bollet C, Fuentes P, Gouin F. Bronchoscopic or blind sampling techniques for the diagnosis of ventilator-associated pneumonia. Am J Respir Crit Care Med. 1995. 152:1982–1991.22. el-Ebiary M, Torres A, González J, de la Bellacasa JP, García C, Jiménez de Anta MT, Ferrer M, Rodriguez-Roisin R. Quantitative cultures of endotracheal aspirates for the diagnosis of ventilator-associated pneumonia. Am Rev Respir Dis. 1993. 148:1552–1557.23. Michel F, Franceschini B, Berger P, Arnal JM, Gainnier M, Sainty JM, Papazian L. Early antibiotic treatment for BAL-confirmed ventilator-associated pneumonia: a role for routine endotracheal aspirate cultures. Chest. 2005. 127:589–597.24. Marquette CH, Georges H, Wallet F, Ramon P, Saulnier F, Neviere R, Mathieu D, Rime A, Tonnel AB. Diagnostic efficiency of endotracheal aspirates with quantitative bacterial cultures in intubated patients with suspected pneumonia. Comparison with the protected specimen brush. Am Rev Respir Dis. 1993. 148:138–144.25. Torres A, Martos A, Puig de la Bellacasa J, Ferrer M, el-Ebiary M, González J, Gené A, Rodríguez-Roisin R. Specificity of endotracheal aspiration, protected specimen brush, and bronchoalveolar lavage in mechanically ventilated patients. Am Rev Respir Dis. 1993. 147:952–957.26. Sauaia A, Moore FA, Moore EE, Haenel JB, Kaneer L, Read RA. Diagnosing pneumonia in mechanically ventilated trauma patients: endotracheal aspirate versus bronchoalveolar lavage. J Trauma. 1993. 35:512–517.27. Jourdain B, Novara A, Joly-Guillou ML, Dombret MC, Calvat S, Trouillet JL, Gibert C, Chastre J. Role of quantitative cultures of endotracheal aspirates in the diagnosis of nosocomial pneumonia. Am J Respir Crit Care Med. 1995. 152:241–246.28. Marquette CH, Copin MC, Wallet F, Neviere R, Saulnier F, Mathieu D, Durocher A, Ramon P, Tonnel AB. Diagnostic tests for pneumonia in ventilated patients: prospective evaluation of diagnostic accuracy using histology as a diagnostic gold standard. Am J Respir Crit Care Med. 1995. 151:1878–1888.29. Wu CL, Yang Dle, Wang NY, Kuo HT, Chen PZ. Quantitative culture of endotracheal aspirates in the diagnosis of ventilator-associated pneumonia in patients with treatment failure. Chest. 2002. 122:662–668.30. Singh N, Rogers P, Atwood CW, Wagener MM, Yu VL. Short-course empiric antibiotic therapy for patients with pulmonary infiltrates in the intensive care unit. A proposed solution for indiscriminate antibiotic prescription. Am J Respir Crit Care Med. 2000. 162:505–511.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Comparative Study of Endotracheal Aspirates and Protected Specimen Brush in the Quantitative Cultures of the Ventilator-Associated Pneumonia
- Incidence of Colonization, Ventilator-Associated Pneumonia as Related to the Type of Endotracheal Suction System in Mechanically Ventilated Patients
- Effects of a Closed Endotracheal Suction System on Oxygen Saturation, Ventilator-Associated Pneumonia, and Nursing Efficacy
- Clinical Features and Outcomes of Ventilator-Associated Pneumonia in Neonatal Intensive Care Unit Patients
- Effects of a Ventilator-associated Pneumonia Prevention Program on Incidence Rate and Endotracheal Colonization
