Comparison of CT and 18F-FDG PET for Detecting Peritoneal Metastasis on the Preoperative Evaluation for Gastric Carcinoma
- Affiliations
-
- 1Department of Diagnostic Radiology, Yonsei University College of Medicine, Seoul, Korea. kimnex@yumc.yonsei.ac.kr
- 2Institute of Gastroenterology, Yonsei University College of Medicine, Seoul, Korea.
- 3Department of Nuclear Medicine, Yonsei University College of Medicine, Seoul, Korea.
- 4Department of Nuclear Medicine, Hallym University College of Medicine, Anyang, Korea.
- 5Department of Surgery, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 1092548
- DOI: http://doi.org/10.3348/kjr.2006.7.4.249
Abstract
OBJECTIVE
The aim of our study was to compare the accuracy of CT and 18F-FDG PET for detecting peritoneal metastasis in patients with gastric carcinoma. MATERIALS AND METHODS: One-hundred-twelve patients who underwent a histologic confirmative exam or treatment (laparotomy, n = 107; diagnostic laparoscopy, n = 4; peritoneal washing cytology, n = 1) were retrospectively enrolled. All the patients underwent CT and 18F-FDG PET scanning for their preoperative evaluation. The sensitivities, specificities and accuracies of CT and 18F-FDG PET imaging for the detection of peritoneal metastasis were calculated and then compared using Fisher's exact probability test (p < 0.05), on the basis of the original preoperative reports. In addition, two board-certified radiologists and two board-certified nuclear medicine physicians independently reviewed the CT and PET scans, respectively. A receiver-operating characteristic curve analysis was performed to compare the diagnostic performance of CT and 18F-FDG PET imaging for detecting peritoneal metastasis. RESULTS: Based on the original preoperative reports, CT and 18F-FDG PET showed sensitivities of 76.5% and 35.3% (p = 0.037), specificities of 91.6% and 98.9% (p = 0.035), respectively, and equal accuracies of 89.3% (p = 1.0). The receptor operating characteristics curve analysis showed a significantly higher diagnostic performance for CT (Az = 0.878) than for PET (Az = 0.686) (p = 0.004). The interobserver agreement for detecting peritoneal metastasis was good (κ value = 0.684) for CT and moderate (κ value = 0.460) for PET. CONCLUSION: For the detection of peritoneal metastasis, CT was more sensitive and showed a higher diagnostic performance than PET, although CT had a relatively lower specificity than did PET.
Keyword
MeSH Terms
-
*Tomography, Emission-Computed
Stomach Neoplasms/*pathology
Sensitivity and Specificity
Retrospective Studies
Radiopharmaceuticals/diagnostic use
ROC Curve
*Positron-Emission Tomography
Peritoneal Neoplasms/*radiography/*radionuclide imaging/*secondary
Middle Aged
Male
Iohexol/analogs & derivatives/diagnostic use
Humans
Fluorodeoxyglucose F18/diagnostic use
Female
Contrast Media
Aged, 80 and over
Aged
Adult
Adolescent
Figure
-
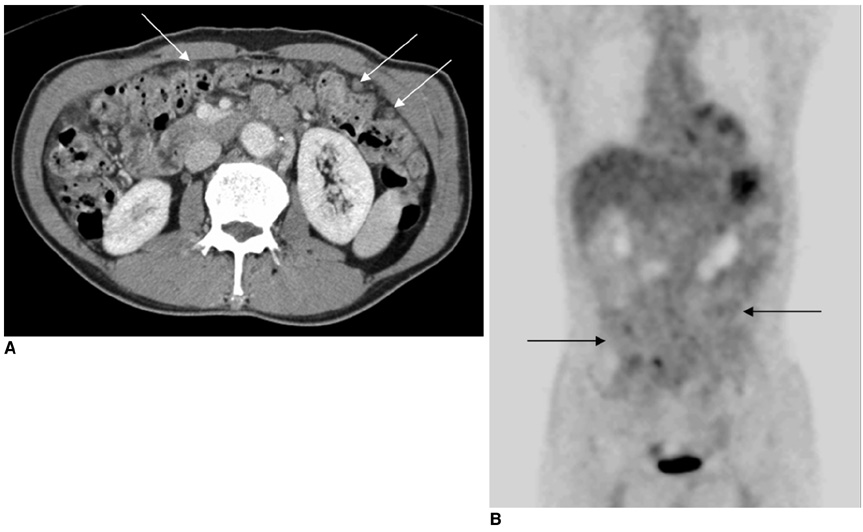
Fig. 1 A 62-year-old man with poorly differentiated adenocarcinoma of the stomach. A. The transverse contrast enhanced CT scan shows multifocal peritoneal implants in the omentum (arrows). B. The PET image shows the diffuse FDG uptake that obscures the visceral outlines in the peritoneal cavity (arrows). Peritoneal metastasis was confirmed by diagnostic laparoscopy.
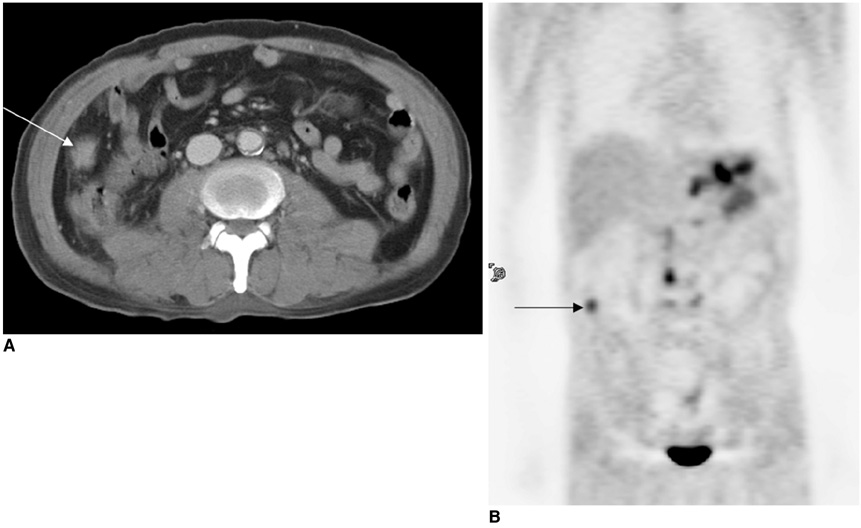
Fig. 2 A 60-year-old man with poorly differentiated adenocarcinoma of the stomach. A. The transverse contrast enhanced CT scan shows a peritoneal implant (arrow) in the right paracolic gutter. B. The PET image shows a discrete focus (arrow) of increased FDG metabolism in the same location. Peritoneal metastasis was confirmed by laparotomy.
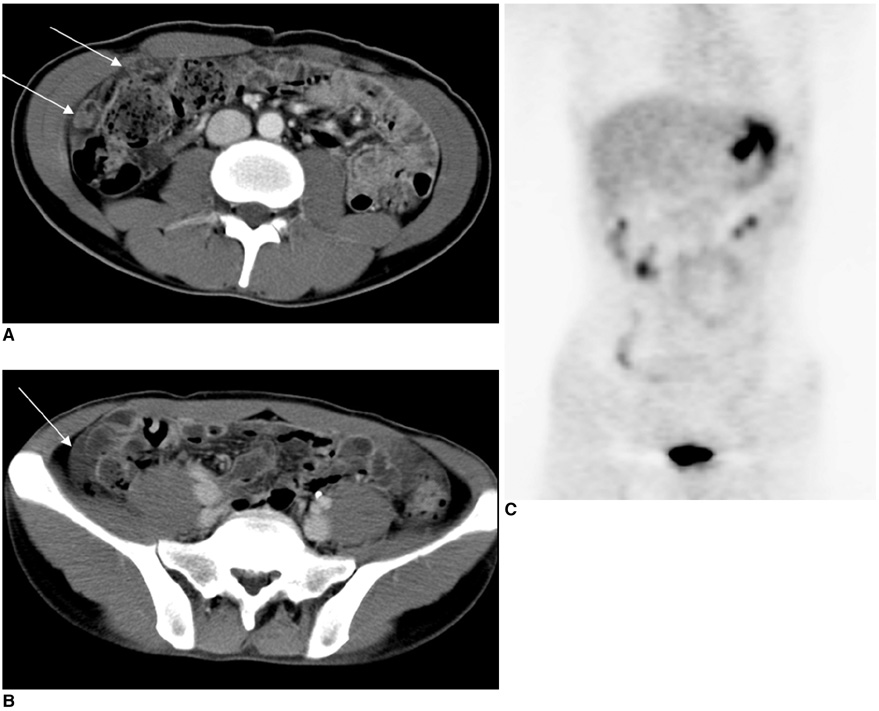
Fig. 3 A 31-year-old man with poorly differentiated adenocarcinoma of the stomach. A. The transverse contrast enhanced CT scan shows multifocal peritoneal implants in the omentum (arrows). B. The transverse CT scan also shows ascitic fluid in the right paracolic gutter (arrows). The CT reviewers interpreted these findings as being highly suggestive of peritoneal metastasis. C. The PET image does not show significantly increased FDG uptake in the peritoneal cavity, except for the normal physiologic colon uptake in the ascending colon. Peritoneal metastasis was confirmed by laparotomy.
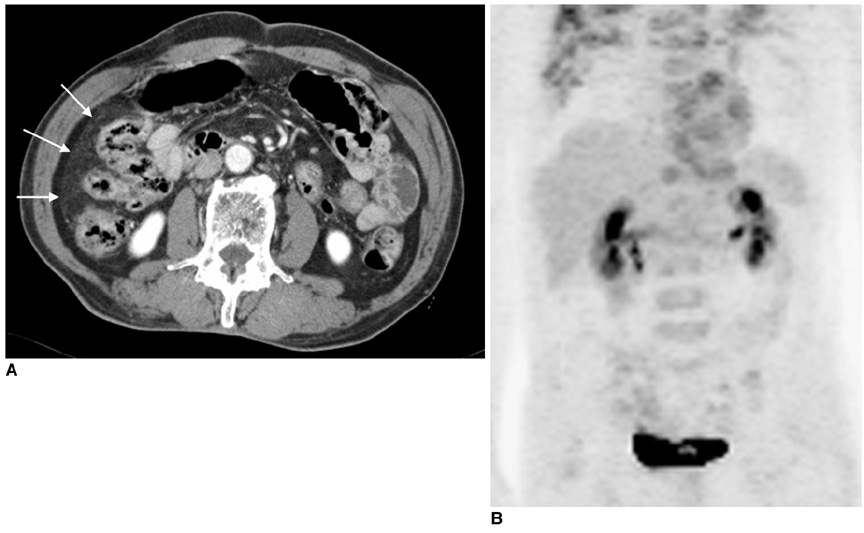
Fig. 4 A 72-year-old man with moderately differentiated adenocarcinoma of the stomach. A. Multiple tiny soft tissue infiltrations are suspected in the right paracolic gutter on the CT image (arrows). The CT reviewers interpreted this finding as being peritoneal metastasis. B. The PET image does not show significantly increased FDG uptake in the peritoneal cavity. The absence of peritoneal metastasis was identified by laparotomy.
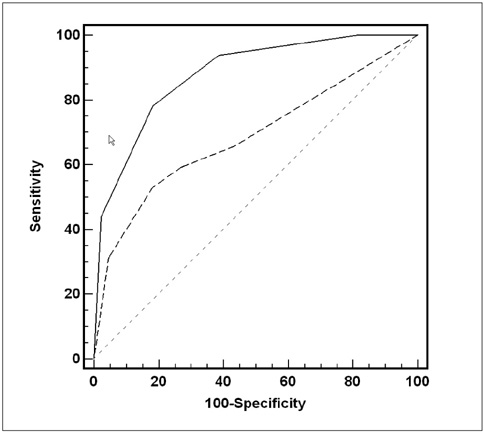
Fig. 5 Plot showing the receiver operating characteristic curves for detecting peritoneal metastasis with using CT (solid line) and PET (dotted line).
Cited by 3 articles
-
Imaging of Gastric Cancer Metabolism Using 18 F-FDG PET/CT
Mijin Yun
J Gastric Cancer. 2014;14(1):1-6. doi: 10.5230/jgc.2014.14.1.1.Role of 18F 2-fluoro-2-deoxyglucose Positron Emission Tomography in Upper Gastrointestinal Malignancies
Hye-Won Yun, Ki-Nam Shim
Korean J Gastroenterol. 2013;61(6):303-306. doi: 10.4166/kjg.2013.61.6.303.Diagnostic performance of F-18 FDG PET or PET/CT for detection of recurrent gastric cancer: a systematic review and meta-analysis
Chang In Choi, Jae Kyun Park, Tae Yong Jeon, Dae-Hwan Kim
J Yeungnam Med Sci. 2023;40(Suppl):S37-S46. doi: 10.12701/jyms.2023.00220.
Reference
-
1. Champault G, Barrat C. Laparoscopy in the staging of cancer of the stomach. J Chir (Paris). 1999. 136:150–155.2. Davies J, Chalmers AG, Sue-Ling HM, May J, Miller GV, Martin IG, et al. Spiral computed tomography and operative staging of gastric carcinoma: a comparison with histopathological staging. Gut. 1997. 41:314–319.3. Dux M, Richter GM, Hansmann J, Kuntz C, Kauffmann GW. Helical hydro-CT for diagnosis and staging of gastric carcinoma. J Comput Assist Tomogr. 1999. 23:913–922.4. Sendler A, Dittler HJ, Feussner H, Nekarda H, Bollschweiler E, Fink U, et al. Preoperative staging of gastric cancer as precondition for multimodal treatment. World J Surg. 1995. 19:501–508.5. Low RN, Barone RM, Lacey C, Sigeti JS, Alzate GD, Sebrechts CP. Peritoneal tumor: MR imaging with dilute oral barium and intravenous gadolinium-containing contrast agents compared with unenhanced MR imaging and CT. Radiology. 1997. 204:513–520.6. Gryspeerdt S, Clabout L, Van Hoe L, Berteloot P, Vergote IB. Intraperitoneal contrast material combined with CT for detection of peritoneal metastases of ovarian cancer. Eur J Gynaecol Oncol. 1998. 19:434–437.7. Boudiaf M, Bedda S, Soyer P, Panis Y, Zidi S, Kardache M, et al. Preoperative evaluation of gastric adenocarcinomas: comparison of CT results with surgical and patholgic results. Ann Chir. 1999. 53:115–122.8. Rohren EM, Turkington TG, Coleman RE. Clinical applications of PET in oncology. Radiology. 2004. 231:305–332.9. Park DH, Kim KH, Park SY, Lee BH, Choi CW, Chin SY. Diagnosis of recurrent uterine cervical cancer: computed tomography versus positron emission tomography. Korean J Radiol. 2000. 1:51–55.10. Kluge R, Schmidt F, Caca K, Barthel H, Hesse S, Georgi P, et al. Positron emission tomography with [(18)F]fluoro-2-deoxy-D-glucose for diagnosis and staging of bile duct cancer. Hepatology. 2001. 33:1029–1035.11. Tanaka T, Kawai Y, Kanai M, Taki Y, Nakamoto Y, Takabayashi A. Usefulness of FDG-positron emission tomography in diagnosing peritoneal recurrence of colorectal cancer. Am J Surg. 2002. 184:433–436.12. Turlakow A, Yeung HW, Salmon AS, Macapinlac HA, Larson SM. Peritoneal carcinomatosis: role of (18)F-FDG PET. J Nucl Med. 2003. 44:1407–1412.13. Buy JN, Moss AA, Ghossain MA, Sciot C, Malbec L, Vadrot D, et al. Peritoneal implants from ovarian tumors: CT findings. Radiology. 1988. 169:691–694.14. Halvorsen RA Jr, Panushka C, Oakley GJ, Letourneau JG, Adcock LL. Intraperitoneal contrast material improves the CT detection of peritoneal metastases. AJR Am J Roentgenol. 1991. 157:37–40.15. Walkey MM, Friedman AC, Sohotra P, Radecki PD. CT manifestations of peritoneal carcinomatosis. AJR Am J Roentgenol. 1988. 150:1035–1041.16. Coakley FV, Choi PH, Gougoutas CA, Pothuri B, Venkatraman E, Chi D, et al. Peritoneal metastases: detection with spiral CT in patients with ovarian cancer. Radiology. 2002. 223:495–499.17. Lin EC, Lear J, Quaife RA. Metastatic peritoneal seeding patterns demonstrated by FDG positron emission tomographic imaging. Clin Nucl Med. 2001. 26:249–250.18. Fleiss J. Statistical methods for rates and proportions. 1981. 2nd ed. New York: Wiley;212–236.19. Tang Y, Yamashita Y, Arakawa A, Namimoto T, Mitsuzaki K, Abe Y, et al. Detection of hepatocellular carcinoma arising in cirrhotic livers: comparison of gadolinium- and ferumoxides-enhanced MR imaging. AJR Am J Roentgenol. 1999. 172:1547–1554.20. Blakeborough A, Ward J, Wilson D, Griffiths M, Kajiya Y, Guthrie JA, et al. Hepatic lesion detection at MR imaging: a comparative study with four sequences. Radiology. 1997. 203:759–765.21. Wang PH, Liu RS, Li YF, Ng HT, Yuan CC. Whole-body PET with (fluorine-18)-2-deoxyglucose for detecting recurrent primary serous peritoneal carcinoma: An initial report. Gynecol Oncol. 2000. 77:44–47.22. Sussman SK, Halvorsen RA Jr, Illescas FF, Cohan RH, Saeed M, Silverman PM, et al. Gastric adenocarcinoma: CT versus surgical staging. Radiology. 1988. 167:335–340.23. Prayer L, Kainz C, Kramer J, Stiglbauer R, Schurawitzki H, Baldt M, et al. CT and MR accuracy in the detection of tumor recurrence in patients treated for ovarian cancer. J Comput Assist Tomogr. 1993. 17:626–632.24. Stahl A, Ott K, Weber WA, Becker K, Link T, Siewert JR, et al. FDG PET imaging of locally advanced gastric carcinomas: correlation with endoscopic and histopathological findings. Eur J Nucl Med Mol Imaging. 2003. 30:288–295.25. Yoshioka T, Yamaguchi K, Kubota K, Saginoya T, Yamazaki T, Ido T, et al. Evaluation of 18F-FDG PET in patients with a, metastatic, or recurrent gastric cancer. J Nucl Med. 2003. 44:690–699.26. Ming SC. Gastric carcinoma. A pathobiological classification. Cancer. 1977. 39:2475–2285.27. Noda S, Soejima K, Inokuchi K. Clinicopathological analysis of the intestinal type and diffuse type of gastric carcinoma. Jpn J Surg. 1980. 10:277–283.28. Sugano H, Nakamura K, Kato Y. Pathological studies of human gastric cancer. Acta Pathol Jpn. 1982. 32:Suppl 2. 329–347.29. De Potter T, Flamen P, Van Cutsem E, Penninckx F, Filez L, Bormans G, et al. Whole-body PET with FDG for the diagnosis of recurrent gastric cancer. Eur J Nucl Med Mol Imaging. 2002. 29:525–529.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- F18-fluorodeoxyglucose-positron emission tomography and computed tomography is not accurate in preoperative staging of gastric cancer
- The Diagnostic Utility of PET-CT for the Preoperative Evaluation of Lymph Node Metastasis in Gastric Cancer Patients
- Use of 18F-FDG PET/CT in Second Primary Cancer
- Late Port Site Metastasis from Occult Gall Bladder Carcinoma After Laparoscopic Cholecystectomy for Cholelithiasis: The Role of 18F-FDG PET/CT
- Supraclavicular Lymph Node Metastasis from Various Malignancies: Assessment with 18F-Fluorodeoxyglucose Positron Emission Tomography/CT, Contrast-Enhanced CT and Ultrasound
