Multidetector CT and MR Imaging of Cardiac Tumors
- Affiliations
-
- 1Department of Radiology and Center for Imaging Science, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul 135-710, Korea. yhchoe@skku.edu
- 2Department of Thoracic and Cardiovascular Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul 135-710, Korea.
- 3Division of Cardiology, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul 135-710, Korea.
- 4Department of Pathology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul 135-710, Korea.
- KMID: 1088728
- DOI: http://doi.org/10.3348/kjr.2009.10.2.164
Abstract
- The purpose of this article is to provide a current review of the spectrum of multidetector CT (MDCT) and MRI findings for a variety of cardiac neoplasms. In the diagnosis of cardiac tumors, the use of MDCT and MRI can help differentiate benign from malignant masses. Especially, the use of MDCT is advantageous in providing anatomical information and MRI is useful for tissue characterization of cardiac masses. Knowledge of the characteristic MRI findings of benign cardiac tumors or thrombi can be helpful to avoid unnecessary surgical procedures. Presurgical assessment of malignant cardiac tumors with the use of MDCT and MRI may allow determination of the resectability of tumors and planning for the reconstruction of cardiac chambers.
MeSH Terms
Figure
-

Fig. 1 Left atrial myxoma in 38-year-old female. A. Reformatted ECG-gated multidetector CT image in 4-chamber view shows mass (arrow) in left atrium. B. Note mass (arrow) extends into left ventricle during diastolic phase through mitral valve.
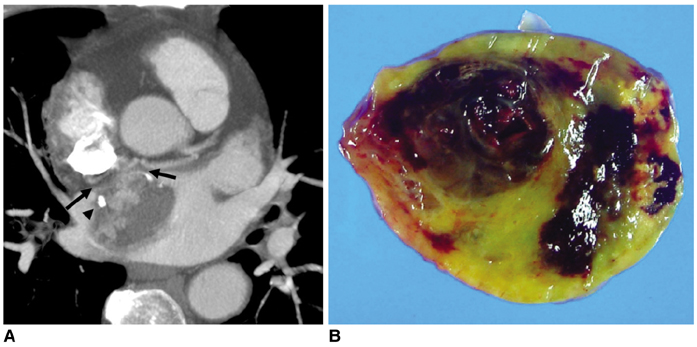
Fig. 2 Left atrial myxoma in 65-year-old male. A. Reformatted ECG-gated multidetector CT image shows left atrial mass attached to interatrial septum by broad pedicle (arrows). Note strong contrast enhancement in part of mass with foci of calcification (arrowhead). B. Gross specimen shows myxoid soft tissue mass with pale yellow and dark brown colors, which probably represent mixture of hemorrhage, necrosis, cyst formation and fibrosis.
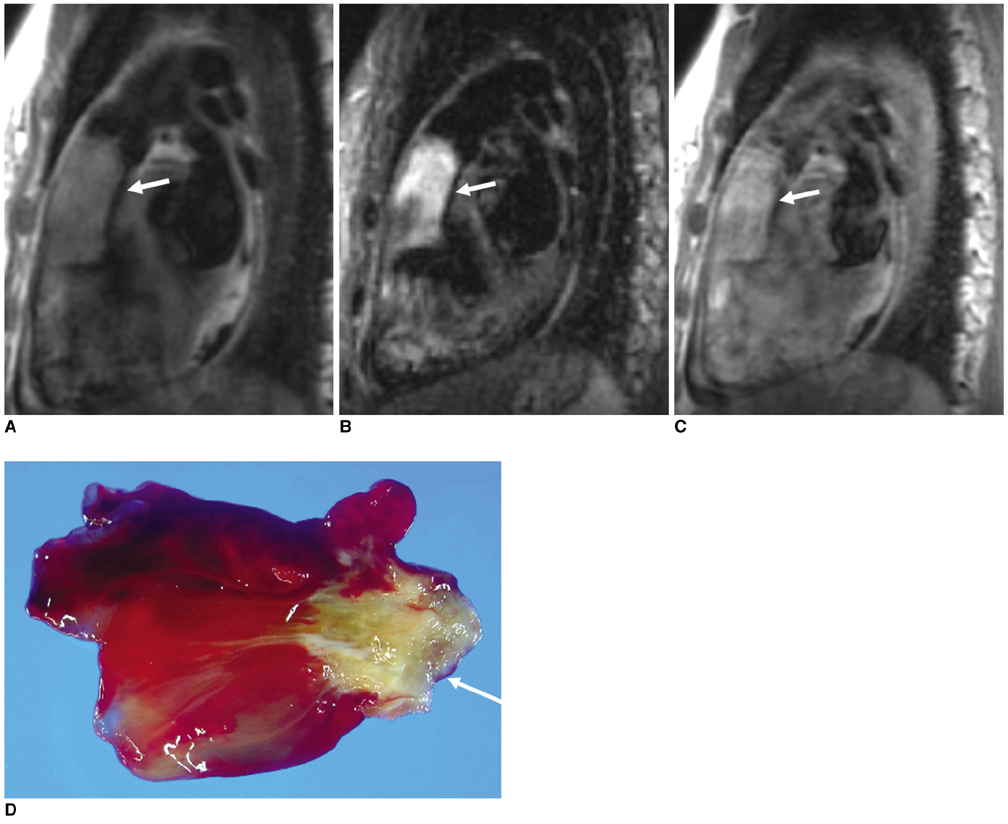
Fig. 3 Right ventricular myxoma in 30-year-old female. A. Sagittal double inversion-recovery MR image demonstrates isointense mass (arrow) occupying right ventricular outflow tract. B. Sagittal triple inversion-recovery image demonstrates bright signal intensity in most parts of mass (arrow). C. Postcontrast double inversion-recovery image demonstrates hyperenhancement of mass (arrow). D. Gross specimen demonstrates yellow soft tissue mass with narrow base of attachment (arrow) to right ventricle.
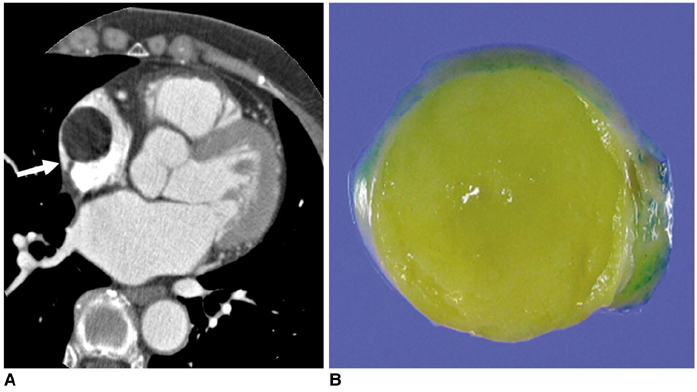
Fig. 4 Right atrial lipoma in 62-year-old female. A. ECG-gated multidetector CT image shows homogeneously low-attenuated mass with pedicle (arrow) attached to free wall of right atrium. B. Gross specimen with cut section shows fatty nature of mass.

Fig. 5 Papillary fibroelastoma of aortic valve in 60-year-old female A. ECG-gated multidetector CT image demonstrates abnormal thickening of aortic valve (arrow). B, C. Oblique cine MR images demonstrates small mass (arrows) attached to aortic valve that was moving according to valvular motion. D. Oblique transverse triple inversion-recovery MR image demonstrates slightly high signal intensity of small mass (arrow). E. Surgical specimen shows small mass with many branching frond-like structures. F. Photomicrograph (Hematoxylin & Eosin staining, ×150) shows fibrous core and scattered smooth muscle cells within papillary projections.
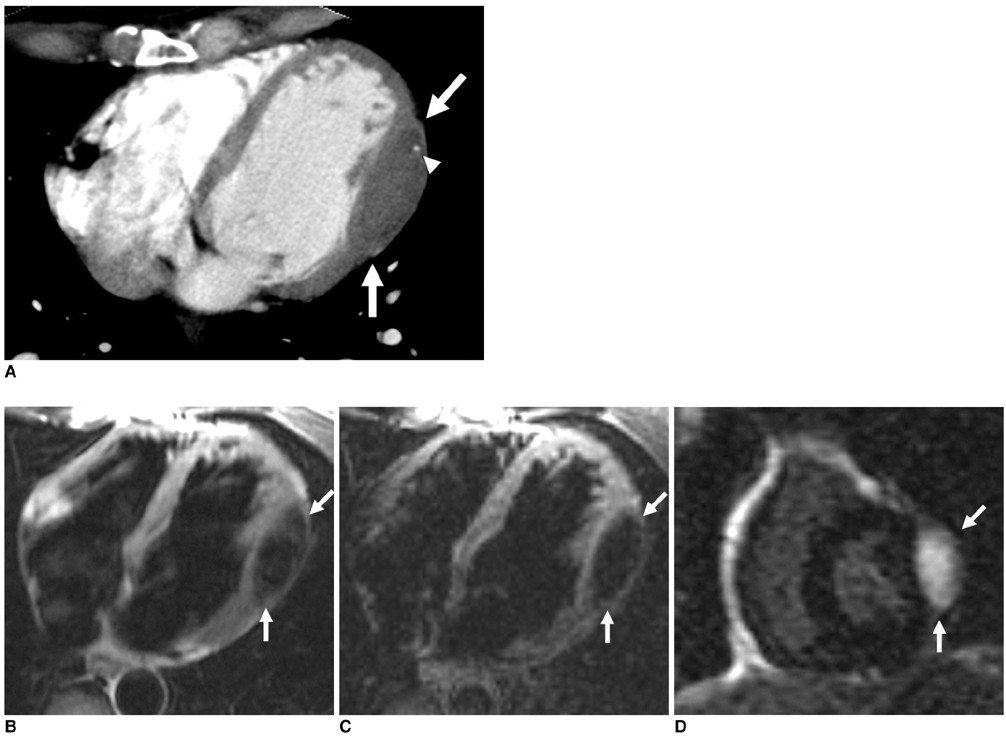
Fig. 6 Left ventricular fibroma in 48-year-old female. A. ECG-gated multidetector CT image shows myocardial thickening (arrows) and spotty calcification (arrowhead) in lateral wall of left ventricle. B. Transverse double inversion-recovery MR image shows hypointense mass (arrows) in myocardium of left ventricle. C. Transverse triple inversion-recovery MR image also shows hypointense mass (arrows) in myocardium of left ventricle. D. Delayed MR image with suppression of normal myocardial signal 10 minutes after administration of gadolinium demonstrates hyperenhancement of mass (arrows).
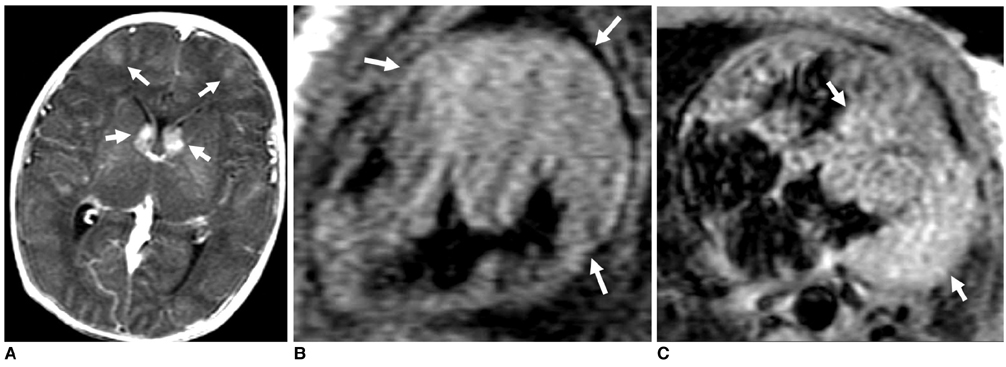
Fig. 7 Cardiac rhabdomyoma in newborn with tuberous sclerosis A. Gadolinium-enhanced T1-weighted MR image shows abnormal enhancing lesions (arrows) in both caudate nuclei and frontal lobes, indicating presence of tubers. B. Sagittal T1-weighted spin echo MR image shows isointense mass (arrows) in septum and anterior wall of left ventricle. C. Transverse gadolinium-enhanced T1-weighted spin echo MR image shows mild enhancement of mass (arrows).
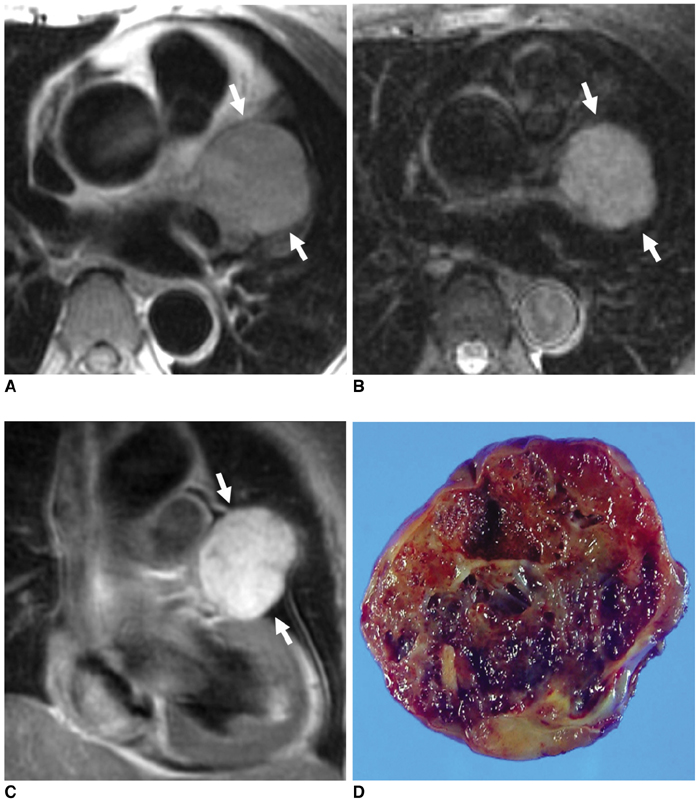
Fig. 8 Cavernous hemangioma of left atrial appendage in 66-year-old female. A. Transverse double inversionrecovery MR image shows intermediate signal intensity mass (arrows) in left atrial appendage. B. Transverse triple inversion-recovery MR image shows hyperintense mass (arrows) with smooth margin. C. Coronal gadolinium-enhanced double inversion-recovery MR image shows strong enhancement of lesion (arrows). D. Gross specimen with cut section demonstrates trabecular, hemorrhagic, and cystic appearance of mass.

Fig. 9 Angiosarcoma of right atrium in 48-year-old male. A. ECG-gated multidetector CT image shows large mass (arrows) in free wall of right atrium. Mass shows irregular and nodular contour and strong contrast enhancement. B. Transverse double inversion-recovery MR image demonstrates mostly isointense mass (arrows) in right atrium. C. Transverse triple inversion-recovery MR image demonstrates presence of heterogeneously hyperintense mass (arrows). D. Gadolinium-enhanced double inversion-recovery MR image shows heterogeneous hyperenhancement of mass. Within mass, some portions (arrows) have no enhancement, representing intratumoral thrombosis. E. Gross specimen shows irregular mass (arrows) of right atrium. Mass had multiple intratumoral thrombi.

Fig. 10 Malignant fibrous histiocytoma in 57-year-old female. A. Transverse double inversion-recovery MR image shows large isointense mass (arrows) arising from posterior wall of left atrium that extends into mitral valve. B. Transverse triple inversion-recovery MR image shows hyperintense mass (arrows) with irregular contour. C. Gadolinium-enhanced double inversion-recovery MR image shows heterogeneous hyperenhancement of mass (arrows). D. ECG-gated multidetector CT reformatted image shows that mitral valve (arrow) is abutting mass. At surgery, mitral valve was found to be involved by malignant mass. Mass was removed and mitral valve was replaced with artificial valve. E. Gross specimen shows presence of multilobulated mass. Cut surface was seen with heterogeneous, gelatinous, myxoid, yellowish white and hemorrhagic appearance (not shown).

Fig. 11 Left atrial myxosarcoma in 72-year-old female. A. Reformatted ECG-gated multidetector CT image shows irregular mass (arrow) with broad-base attachment to left atrium. Also, note minimal wall thickening (arrowheads) of interatrial septum due to tumor spread along left atrial wall and septum. B. Oblique double inversion-recovery MR image depicts hyperintense lesion (arrow) after gadolinium injection. C. Virtual angioscopic multidetector CT image shows irregular mass (arrow) near mitral valve (MV) and small polypoid mass (arrowhead). D. At surgery, presence of lobulated soft tissue mass (arrow) and small polypoid lesions were demonstrated (arrowheads).

Fig. 12 Primary cardiac lymphoma (diffuse large B-cell type) in 73-year-old male. A. Non-gated postcontrast multidetector CT image shows homogeneous and mildly hyperattenuated mass (arrows) in right atrial wall and interatrial septum. Mass is spreading along pericardial space. Pericardial effusion (asterisk) is probably due to pericardial invasion. B. Coronal gadolinium-enhanced double inversion-recovery MR image shows presence of diffuse infiltrative mass (arrows) in right atrium. Mass shows homogeneous enhancement that distinguishes it from pericardial effusion (asterisk).
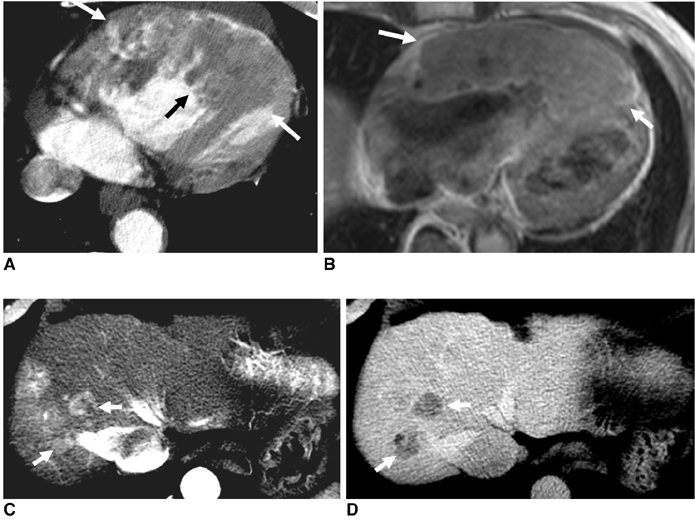
Fig. 13 Hematogenous cardiac metastases from hepatocellular carcinomas in 50-year-old male. A. ECG-gated multidetector CT image shows marked thickening of right ventricular free wall (arrows). B. Gadolinium-enhanced transverse double inversion-recovery MR image shows diffuse thickening of right ventricular wall (arrows). C, D. Arterial (C) and delayed (D) CT images show multiple hepatocellular carcinomas with characteristic dynamic pattern of early enhancement and wash out (arrows).
Reference
-
1. Sutsch G, Jenni R, von Segesser L, Schneider J. Heart tumors: incidence, distribution, diagnosis. Exemplified by 20,305 echocardiographies. Schweiz Med Wochenschr. 1991. 121:621–629.2. McAllister HA Jr, Fenoglio JJ Jr. Tumors of the cardiovascular system. Atlas of tumor pathology. 1978. 2nd ed. Washington, DC: Armed Forces Institute of Pathology;15.3. Araoz PA, Eklund HE, Welch TJ, Breen JF. CT and MR imaging of primary cardiac malignancies. Radiographics. 1999. 19:1421–1434.4. Hong C, Becker CR, Huber A, Schoepf UJ, Ohnesorge B, Knez A, et al. ECG-gated reconstructed multi-detector row CT coronary angiography: effect of varying trigger delay on image quality. Radiology. 2001. 220:712–717.5. Burke A, Virmani R. Tumors of the heart and great vessels. Atlas of tumor pathology. 1996. 3rd ed. Washington, DC: Armed Forces Institute of Pathology;79–90.6. Moriyama Y, Saigenji H, Shimokawa S, Toyohira H, Taira A. The surgical treatment of 30 patients with cardiac myxomas: a comparison of clinical features according to morphological classification. Surg Today. 1994. 24:596–598.7. Grebenc ML, Rosado-de-Christenson ML, Green CE, Burke AP, Galvin JR. Cardiac myxoma: imaging features in 83 patients. Radiographics. 2002. 22:673–689.8. Masui T, Takahashi M, Miura K, Naito M, Tawarahara K. Cardiac myxoma: identification of intratumoral hemorrhage and calcification on MR images. AJR Am J Roentgenol. 1995. 164:850–852.9. Edwards FH, Hale D, Cohen A, Thompson L, Pezzella AT, Virmani R. Primary cardiac valve tumors. Ann Thorac Surg. 1991. 52:1127–1131.10. Burke AP, Rosado-de-Christenson M, Templeton PA, Virmani R. Cardiac fibroma: clinicopathologic correlates and surgical treatment. J Thorac Cardiovasc Surg. 1994. 108:862–870.11. De Cobelli F, Esposito A, Mellone R, Papa M, Varisco T, Besana R, et al. Images in cardiovascular medicine. Late enhancement of a left ventricular cardiac fibroma assessed with gadolinium-enhanced cardiovascular magnetic resonance. Circulation. 2005. 112:E242–E243.12. Webb DW, Thomas RD, Osborne JP. Cardiac rhabdomyomas and their association with tuberous sclerosis. Arch Dis Child. 1993. 68:367–370.13. Newell JD 2nd, Eckel C, Davis M, Tadros NB. MR appearance of an arteriovenous hemangioma of the interventricular septum. Cardiovasc Intervent Radiol. 1988. 11:319–321.14. Yahata S, Endo T, Honma H, Ino T, Hayakawa H, Ogawa M, et al. Sunray appearance on enhanced magnetic resonance image of cardiac angiosarcoma with pericardial obliteration. Am Heart J. 1994. 127:468–471.15. Okamoto K, Kato S, Katsuki S, Wada Y, Toyozumi Y, Morimatsu M, et al. Malignant fibrous histiocytoma of the heart: case report and review of 46 cases in the literature. Intern Med. 2001. 40:1222–1226.16. Awamleh P, Alberca MT, Gamallo C, Enrech S, Sarraj A. Left atrium myxosarcoma: an exceptional cardiac malignant primary tumor. Clin Cardiol. 2007. 30:306–308.17. Dorsay TA, Ho VB, Rovira MJ, Armstrong MA, Brissette MD. Primary cardiac lymphoma: CT and MR findings. J Comput Assist Tomogr. 1993. 17:978–981.18. Lam KY, Dickens P, Chan AC. Tumors of the heart. A 20-year experience with a review of 12,485 consecutive autopsies. Arch Pathol Lab Med. 1993. 117:1027–1103.19. Klatt EC, Heitz DR. Cardiac metastases. Cancer. 1990. 65:1456–1459.20. Sparrow PJ, Kurian JB, Jones TR, Sivananthan MU. MR imaging of cardiac tumors. Radiographics. 2005. 25:1255–1276.21. Gaerte SC, Meyer CA, Winer-Muram HT, Tarver RD, Conces DJ Jr. Fat-containing lesions of the chest. Radiographics. 2002. 22:S61–S78.22. Hoffmann U, Globits S, Frank H. Cardiac and paracardiac masses. Current opinion on diagnostic evaluation by magnetic resonance imaging. Eur Heart J. 1998. 19:553–563.23. Hansen MW, Merchant N. MRI of hypertrophic cardiomyopathy: part I, MRI appearances. AJR Am J Roentgenol. 2007. 189:1335–1343.24. Mirowitz SA, Gutierrez FR. Fibromuscular elements of the right atrium: pseudomass at MR imaging. Radiology. 1992. 182:231–233.25. Gaudio C, Di Michele S, Cera M, Nguyen BL, Pannarale G, Alessandri N. Prominent crista terminalis mimicking a right atrial mixoma: cardiac magnetic resonance aspects. Eur Rev Med Pharmacol Sci. 2004. 8:165–168.26. Paydarfar D, Krieger D, Dib N, Blair RH, Pastore JO, Stetz JJ Jr, et al. In vivo magnetic resonance imaging and surgical histopathology of intracardiac masses: distinct features of subacute thrombi. Cardiology. 2001. 95:40–47.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- CT-Based Essential Cardiac Anatomy for Radiology Residents to Understand Congenital Heart Disease
- Preparation, Technique, and Imaging of Computed Tomography/Magnetic Resonance Enterography
- Detection of Acute Intraventricular Hemorrhage: Comparison of FLAIR MR Imaging with Unenhanced CT
- Aortic Stenosis: Evaluation with Multidetector CT Angiography and MR Imaging
- Coronary Angiography with Multidetector row Computed Tomography: Part I - Technical Aspects
