Prenatal MRI Findings of Fetuses with Congenital High Airway Obstruction Sequence
- Affiliations
-
- 1Department of Radiology, Cincinnati Children's Hospital Medical Center, Cincinnati OH 45229-3039, USA. carolina.guimaraes@cchmc.org
- 2Division of Surgery, Cincinnati Children's Hospital Medical Center, Cincinnati OH 45229-3039, USA.
- 3Division of Genetics, Cincinnati Children's Hospital Medical Center, Cincinnati OH 45229-3039, USA.
- KMID: 1088723
- DOI: http://doi.org/10.3348/kjr.2009.10.2.129
Abstract
OBJECTIVE
To define the MRI findings of congenital high airway obstruction sequence (CHAOS) in a series of fetuses.
MATERIALS AND METHODS
Prenatal fetal MR images were reviewed in seven fetuses with CHAOS at 21 to 27 weeks of gestation. The MRI findings were reviewed. The MRI parameters evaluated included the appearance of the lungs and diaphragm, presence or absence of hydrops, amount of amniotic fluid, airway appearance, predicted level of airway obstruction, and any additional findings or suspected genetic syndromes.
RESULTS
All the fetuses viewed (7 of 7) demonstrated the following MRI findings: dilated airway below the level of obstruction, increased lung signal, markedly increased lung volumes with flattened or inverted hemidiaphragms, massive ascites, centrally positioned and compressed heart, as well as placentomegaly. Other frequent findings were anasarca (6 of 7) and polyhydramnios (3 of 7). MRI identified the level of obstruction as laryngeal in five cases and tracheal in two cases. In four of the patients, surgery or autopsy confirmed the MRI predicted level of obstruction. Associated abnormalities were found in 4 of 7 (genetic syndromes in 2). Postnatal radiography (n = 3) showed markedly hyperinflated lungs with inverted or flattened hemidiaphragms, strandy perihilar opacities, pneumothoraces and tracheotomy. Two fetuses were terminated and one fetus demised in utero. Four fetuses were delivered via ex utero intrapartum treatment procedure.
CONCLUSION
MRI shows a consistent pattern of abnormalities in fetuses with CHAOS, accurately identifies the level of airway obstruction, and helps differentiate from other lung abnormalities such as bilateral congenital pulmonary airway malformation by demonstrating an abnormally dilated airway distal to the obstruction.
MeSH Terms
Figure
-
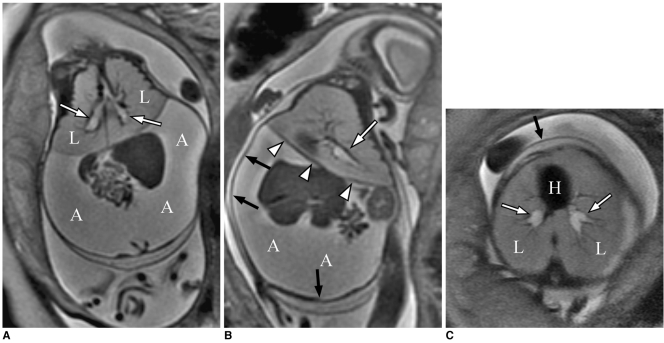
Fig. 1 27-week-old fetus with congenital high airway obstruction sequence.A. Coronal T2-weighted single shot fast spin echo image shows markedly enlarged lung volumes (L) and increase in lung signal, marked ascites (A), and dilated bronchi bilaterally (arrows).B. Sagittal T2-weighted single shot fast spin echo image once again shows inverted diaphragm (arrowheads), ascites (A), dilated bronchus (arrow) and subcutaneous edema (black arrows).C. Axial T2-weighted single shot fast spin echo image shows centrally positioned and compressed heart (H), dilated bronchi (arrows), large lung volumes (L), and subcutaneous edema (black arrow).
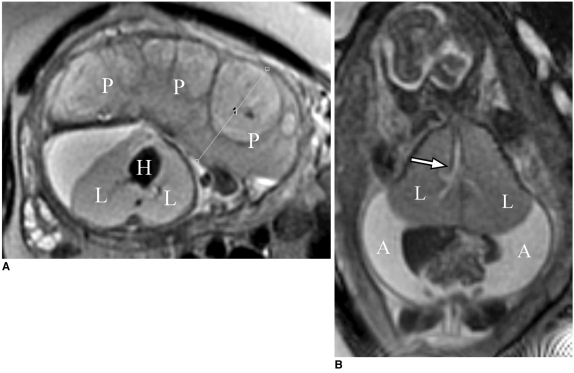
Fig. 2 22-week-old fetus with congenital high airway obstruction sequence.A. Axial T2-weighted single shot fast spin echo image shows marked placentomegaly (P). Note that fetus has centrally positioned and compressed heart (H), and large lung volumes (L).B. Coronal T2-weighted single shot fast spin echo image shows markedly enlarged lung volumes (L) and increase in lung signal, marked ascites (A), and dilated airway (arrow). Note inverted diaphragms.
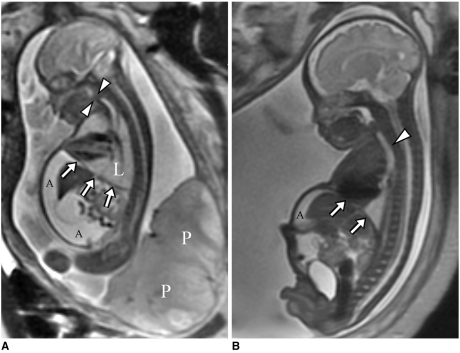
Fig. 3 Congenital high airway obstruction sequence with decreased imaging findings on follow up fetal MR imaging.A. Sagittal T2-weighted single shot fast spin echo image obtained at 23-weeks of gestation shows markedly enlarged lung volumes (L) and increased lung signal, marked ascites (A), and inverted diaphragms (arrows). Note gap seen in fluid-filled, high-signal airway (arrowheads) at level of larynx, consistent with level of obstruction.B. Sagittal T2-weighted single shot fast spin echo image obtained at 33-weeks of gestation shows marked interval reduction in degree of ascites (A), marked decrease in lung volume with resolution of inverted diaphragm (arrows). Gap seen in fluid-filled, high-signal airway at level of larynx is still seen. However, airway distal to level of obstruction (arrowhead) remains dilated.

Fig. 4 Radiograph of chest and abdomen in 1-day-old child with congenital high airway obstruction sequence, delivered by ex utero intrapartum treatment to tracheostomy. Note markedly hyperinflated lungs with flattened hemidiaphragms, strandy perihilar opacities, pneumothoraces, tracheotomy, and enlarged abdomen, which is likely due to ascites. Child expired at 2-months of age.
Cited by 1 articles
-
Perinatal outcome of fetuses with congenital high airway obstruction syndrome: a single-center experience
Sang-Hee Jeong, Mi-Young Lee, Ok-Ju Kang, Rina Kim, Jin-Hoon Chung, Hye-Sung Won, Pil-Ryang Lee, Euiseok Jung, Byong Sop Lee, Woo-Jong Choi, Yoon Se Lee
Obstet Gynecol Sci. 2021;64(1):52-61. doi: 10.5468/ogs.20266.
Reference
-
1. Hedrick MH, Ferro MM, Filly RA, Flake AW, Harrison MR, Adzick NS. Congenital high airway obstruction syndrome (CHAOS): a potential for perinatal intervention. J Pediatr Surg. 1994; 29:271–274. PMID: 8176604.
Article2. Lim FY, Crombleholme TM, Hedrick HL, Flake AW, Johnson MP, Howell LJ, et al. Congenital high airway obstruction syndrome: natural history and management. J Pediatr Surg. 2003; 38:940–945. PMID: 12778398.
Article3. Shimabukuro F, Sakumoto K, Masamoto H, Asato Y, Yoshida T, Shinhama A, et al. A case of congenital high airway obstruction syndrome managed by ex utero intrapartum treatment: case report and review of the literature. Am J Perinatol. 2007; 24:197–201. PMID: 17372858.
Article4. DeCou JM, Jones DC, Jacobs HD, Touloukian RJ. Successful ex utero intrapartum treatment (EXIT) procedure for congenital high airway obstruction syndrome (CHAOS) owing to laryngeal atresia. J Pediatr Surg. 1998; 33:1563–1565. PMID: 9802816.
Article5. Crombleholme TM, Sylvester K, Flake AW, Adzick NS. Salvage of a fetus with congenital high airway obstruction syndrome by ex utero intrapartum treatment (EXIT) procedure. Fetal Diagn Ther. 2000; 15:280–282. PMID: 10971081.
Article6. Paek BW, Callen PW, Kitterman J, Feldstein VA, Farrell J, Harrison MR, et al. Successful fetal intervention for congenital high airway obstruction syndrome. Fetal Diagn Ther. 2002; 17:272–276. PMID: 12169810.
Article7. Kohl T, Hering R, Bauriedel G, Van de Vondel P, Heep A, Keiner S, et al. Fetoscopic and ultrasound-guided decompression of the fetal trachea in a human fetus with Fraser syndrome and congenital high airway obstruction syndrome (CHAOS) from laryngeal atresia. Ultrasound Obstet Gynecol. 2006; 27:84–88. PMID: 16308883.
Article8. Onderoglu L, Saygan Karamursel B, Bulun A, Kale G, Tuncbilek E. Prenatal diagnosis of laryngeal atresia. Prenat Diagn. 2003; 23:277–280. PMID: 12673628.9. Shum DJ, Clifton MS, Coakley FV, Hornberger LK, Joe BN, Goldstein RB, et al. Prenatal tracheal obstruction due to double aortic arch: a potential mimic of congenital high airway obstruction syndrome. AJR Am J Roentgenol. 2007; 188:W82–W85. PMID: 17179331.
Article10. Kuwashima S, Kitajima K, Kaji Y, Watanabe H, Watabe Y, Suzumura H. MR imaging appearance of laryngeal atresia (congenital high airway obstruction syndrome): unique course in a fetus. Pediatr Radiol. 2008; 38:344–347. PMID: 18071686.
Article11. Ulreich S, Gruslin A, Nodell CG, Pretorius DH. Nyberg DA, McGahan JP, Pretorius DH, Pilu G, editors. Fetal hydrops and ascites. Diagnostic imaging of fetal anomalies. 2003. Philadelphia: Lippincott Williams & Wilkins;p. 713.12. Sepulveda W, Sebire NJ, Harris R, Nyberg DA. Nyberg DA, McGahan JP, Pretorius DH, Pilu G, editors. The placenta, umbilical cord, and membranes. Diagnostic imaging of fetal anomalies. 2003. Philadelphia: Lippincott Williams & Wilkins;p. 85.13. Davey MG, Hooper SB, Tester ML, Johns DP, Harding R. Respiratory function in lambs after in utero treatment of lung hypoplasia by tracheal obstruction. J Appl Physiol. 1999; 87:2296–2304. PMID: 10601181.14. Mychaliska GB, Bealer JF, Graf JL, Rosen MA, Adzick NS, Harrison MR. Operating on placental support: the ex utero intrapartum treatment procedure. J Pediatr Surg. 1997; 32:227–230. PMID: 9044127.
Article15. Berg C, Geipel A, Germer U, Pertersen-Hansen A, Koch-Dorfler M, Gembruch U. Prenatal detection of Fraser syndrome without cryptophthalmos: case report and review of the literature. Ultrasound Obstet Gynecol. 2001; 18:76–80. PMID: 11489232.
Article16. Hartnick CJ, Rutter M, Lang F, Willging JP, Cotton RT. Congenital high airway obstruction syndrome and airway reconstruction: an evolving paradigm. Arch Otolaryngol Head Neck Surg. 2002; 128:567–570. PMID: 12003589.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Usefulness of Fetal MRI for Prenatal Diagnosis
- Perinatal outcome of fetuses with congenital high airway obstruction syndrome: a single-center experience
- A case of congenital high airway obstruction syndrome caused by complete tracheal obstruction with associated anomalies
- Significance of prenatal radiologic diagnosis of the central nervous system anomalies
- A Case of the Ex Utero Intrapartum Treatment in Congenital Fetal Oral Teratoma
