Evaluation of Reperfused Myocardial Infarction by Low-Dose Multidetector Computed Tomography Using Prospective Electrocardiography (ECG)-Triggering: Comparison with Magnetic Resonance Imaging
- Affiliations
-
- 1Department of Radiology and Research Institute of Radiological Science, Gangnam Severance Hospital, Yonsei University College of Medicine, Seoul, Korea. thkim1@yuhs.ac
- 2Department of Cardiology, Gangnam Severance Hospital, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 1071419
- DOI: http://doi.org/10.3349/ymj.2010.51.5.683
Abstract
- PURPOSE
To evaluate the potential of prospective electrocardiography (ECG)-gated 64-slice multidetector computed tomography (MDCT) for evaluation of myocardial enhancement, infarct size, and stent patency after percutaneous coronary intervention (PCI) with stenting in patients with myocardial infarction.
MATERIALS AND METHODS
Seventeen patients who were admitted with acute myocardial infarction were examined with prospective ECG-gated 64-slice cardiac MDCT and magnetic resonance (MR) imaging after reperfusion using PCI with stenting. Cardiac MDCT was performed with two different phases: arterial and delayed phases. We evaluated the stent patency on the arterial phase, and nonviable myocardium on the delayed phase of computed tomography (CT) image, and they were compared with the results from the delayed MR images.
RESULTS
Total mean radiation dose was 7.7 +/- 0.5 mSv on the two phases of CT images. All patients except one showed good patency of the stent at the culprit lesion on the arterial phase CT images. All patients had hyperenhanced area on the delayed phase CT images, which correlated well with those on the delayed phase MR images, with a mean difference of 1.6% (20 +/- 10% vs. 22 +/- 10%, r = 0.935, p = 0.10). Delayed MR images had a better contrast-to-noise ratio (CNR) than delayed CT images (27.1 +/- 17.8% vs. 4.3 +/- 2.1%, p < 0.001).
CONCLUSION
Prospective ECG-gated 64-slice MDCT provides the potential to evaluate myocardial viability on delayed phase as well as for stent patency on arterial phase with an acceptable radiation dose after PCI with stenting in patients with myocardial infarction.
Keyword
MeSH Terms
Figure
-

Fig. 1 Images obtained for a 50-year-old man with anterolateral myocardial infarction. (A) Total occlusion in the ramus intermedius (RI) (arrow) and 60% stenosis in the mid-LAD artery. (B and C) Patent stents at the culprit lesion of RI and the LAD artery on 3D-VRT (A) and curved MPR (C) CT images after PCI with stenting. (D-F) No definite area of hypoperfusion and some beam-hardening artifact in anterior and posterior wall of left ventricle on the arterial CT image (D), anterolateral hyperenhancement on delayed phase CT (E) (white arrows) and MR (F) images. LAD, left anterior descending artery; 3D-VRT, 3 dimensional volume rendering technique; MPR, multiplannar reformatted imaged; CT, computed tomography; PCI, percutaneous coronary intervention. LAD, left anterior descending artery; 3D-VRT, 3-dimensional volume rendering technique; MPR, multiplannar reformatted imaged; CT, computed tomography; PCI, percutaneous coronary intervention; MR, magnetic resonance.
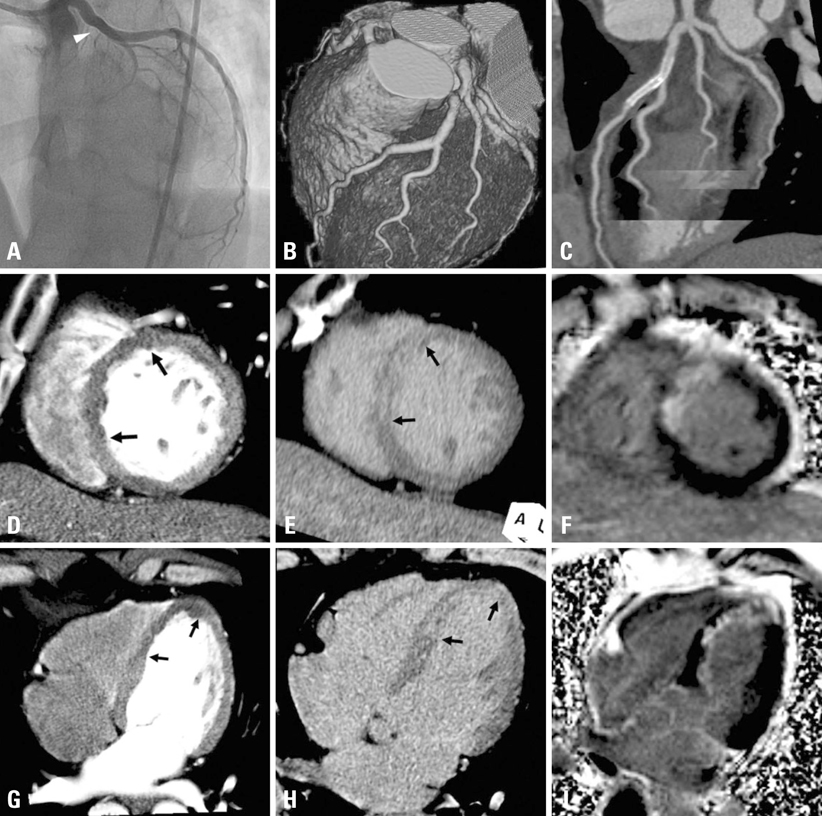
Fig. 2 Images obtained for a 59-year-old man with anteroseptal myocardial infarction. (A) Total occlusion at ostium of the LAD artery (arrowhead). (B and C) A patent stent at the culprit lesion of LAD artery on 3D-VRT (B) and curved MPR (C) CT images after PCI with stenting. (D-I) Anteroseptal hypoperfusion on early arterial CT images (D-G) (arrows), anteroseptal hyperenhancement on delayed phase CT (E-H) (arrows) and MR (F-I) images. LAD, left anterior descending artery; 3D-VRT, 3-dimensional volume rendering technique; MPR, multiplannar reformatted imaged; CT, computed tomography; PCI, percutaneous coronary intervention; MR, magnetic resonance.
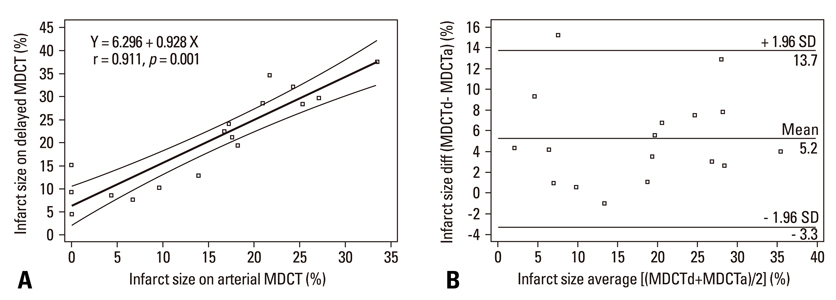
Fig. 3 Linear regression analysis and Bland-Altman plots for infarct size between early arterial and delayed phase MDCT images. (A) Areas of hypoperfusion and hyperenhancement for early arterial phase and delayed phase MDCT images (Y = 6.296 + 0.928X, r = 0.911, p < 0.001). (B) Bland-Altman plots showing the relationship between early arterial MDCT images and delayed enhanced MDCT images. Mean differences (y-axes) between each pair [(mean MDCTd) - (mean MDCTa)] are plotted against the average values (x-axes) of the same pair [{(mean MDCTd) + (mean MDCTa)}/2]. These results showed that area of hyperenhancement on the delayed phase MDCT images was 5.2% larger than that of hypoenhancement on the arterial phase MDCT images (p < 0.05). MDCTd (a) = multidetector computed tomography, arterial phase (delayed phase). MDCT, multidetector computed tomography.
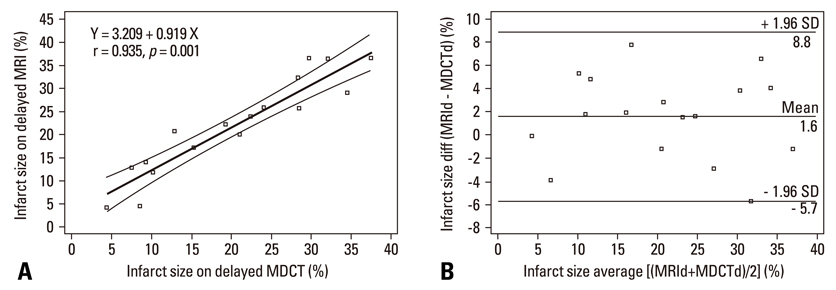
Fig. 4 Linear regression analysis and Bland-Altman plots for infarct size between delayed phase MDCT images and delayed phase MR images. (A) Areas of hyperenhancement for delayed phase MDCT and MR images (Y = 3.209 + 0.919X, r = 0.935, p < 0.001). (B) Bland-Altman plots showing the relationships between delayed enhanced MDCT and MR images. Mean differences (y-axes) between each pair [(mean MRId) - (mean MDCTd)] are plotted against the average values (x-axes) of the same pair [{(mean MRId) + (mean MDCTd)}/2]. These results showed that the delayed phase MDCT infarct size was 1.6% larger than MRI (p = 0.10). MDCT, multidetector computed tomography.
Reference
-
1. Gutberlet M, Fröhlich M, Mehl S, Amthauer H, Hausmann H, Meyer R, et al. Myocardial viability assessment in patients with highly impaired left ventricular function: comparison of delayed enhancement, dobutamine stress MRI, end-diastolic wall thickness, and TI201-SPECT with functional recovery after revascularization. Eur Radiol. 2005. 15:872–880.
Article2. Lardo AC, Cordeiro MA, Silva C, Amado LC, George RT, Saliaris AP, et al. Contrast-enhanced multidetector computed tomography viability imaging after myocardial infarction: characterization of myocyte death, microvascular obstruction, and chronic scar. Circulation. 2006. 113:394–404.
Article3. Kühl HP, Papavasiliu TS, Beek AM, Hofman MB, Heusen NS, van Rossum AC. Myocardial viability: rapid assessment with delayed contrast-enhanced MR imaging with three-dimensional inversion-recovery prepared pulse sequence. Radiology. 2004. 230:576–582.
Article4. Kim RJ, Wu E, Rafael A, Chen EL, Parker MA, Simonetti O, et al. The use of contrast-enhanced magnetic resonance imaging to identify reversible myocardial dysfunction. N Engl J Med. 2000. 343:1445–1453.
Article5. Nieman K, Cademartiri F, Lemos PA, Raaijmakers R, Pattynama PM, de Feyter PJ. Reliable noninvasive coronary angiography with fast submillimeter multislice spiral computed tomography. Circulation. 2002. 106:2051–2054.
Article6. Mollet NR, Cademartiri F, van Mieghem CA, Runza G, McFadden EP, Baks T, et al. High-resolution spiral computed tomography coronary angiography in patients referred for diagnostic conventional coronary angiography. Circulation. 2005. 112:2318–2323.
Article7. Achenbach S, Ulzheimer S, Baum U, Kachelriess M, Ropers D, Giesler T, et al. Noninvasive coronary angiography by retrospectively ECG-gated multislice spiral CT. Circulation. 2000. 102:2823–2828.
Article8. Chiou KR, Liu CP, Peng NJ, Huang WC, Hsiao SH, Huang YL, et al. Identification and viability assessment of infarcted myocardium with late enhancement multidetector computed tomography: comparison with thallium single photon emission computed tomography and echocardiography. Am Heart J. 2008. 155:738–745.
Article9. Sato A, Hiroe M, Nozato T, Hikita H, Ito Y, Ohigashi H, et al. Early validation study of 64-slice multidetector computed tomography for the assessment of myocardial viability and the prediction of left ventricular remodelling after acute myocardial infarction. Eur Heart J. 2008. 29:490–498.
Article10. Nieman K, Shapiro MD, Ferencik M, Nomura CH, Abbara S, Hoffmann U, et al. Reperfused myocardial infarction: contrast-enhanced 64-Section CT in comparison to MR imaging. Radiology. 2008. 247:49–56.
Article11. Husmann L, Valenta I, Gaemperli O, Adda O, Treyer V, Wyss CA, et al. Feasibility of low-dose coronary CT angiography: first experience with prospective ECG-gating. Eur Heart J. 2008. 29:191–197.
Article12. Shuman WP, Branch KR, May JM, Mitsumori LM, Lockhart DW, Dubinsky TJ, et al. Prospective versus retrospective ECG gating for 64-detector CT of the coronary arteries: comparison of image quality and patient radiation dose. Radiology. 2008. 248:431–437.
Article13. Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet. 1986. 1:307–310.
Article14. Büecker A, Katoh M, Krombach GA, Spuentrup E, Bruners P, Gunther RW, et al. A feasibility study of contrast enhancement of acute myocardial infarction in multislice computed tomography: comparison with magnetic resonance imaging and gross morphology in pigs. Invest Radiol. 2005. 40:700–704.15. Brodoefel H, Reimann A, Klumpp B, Fenchel M, Ohmer M, Miller S, et al. Assessment of myocardial viability in a reperfused porcine model: evaluation of different MSCT contrast protocols in acute and subacute infarct stages in comparison with MRI. J Comput Assist Tomogr. 2007. 31:290–298.16. Baks T, Cademartiri F, Moelker AD, van der Giessen WJ, Krestin GP, Duncker DJ, et al. Assessment of acute reperfused myocardial infarction with delayed enhancement 64-MDCT. Am J Roentgenol. 2007. 188:W135–W137.
Article17. Mahnken AH, Koos R, Katoh M, Wildberger JE, Spuentrup E, Buecker A, et al. Assessment of myocardial viability in reperfused acute myocardial infarction using 16-slice computed tomography in comparison to magnetic resonance imaging. J Am Coll Cardiol. 2005. 45:2042–2047.
Article18. Trabold T, Buchgeister M, Kuttner A, Heuschmid M, Kopp AF, Schröder S, et al. Estimation of radiation exposure in 16-detector row computed tomography of the heart with retrospective ECG-gating. Rofo. 2003. 175:1051–1055.
Article19. Hirai N, Horiguchi J, Fujioka C, Kiguchi M, Yamamoto H, Matsuura N, et al. Prospective versus retrospective ECG-gated 64-detector coronary CT angiography: assessment of image quality, stenosis, and radiation dose. Radiology. 2008. 248:424–430.20. Giesler T, Baum U, Ropers D, Ulzheimer S, Wenkel E, Mennicke M, et al. Noninvasive visualization of coronary arteries using contrast-enhanced multidetector CT: influence of heart rate on image quality and stenosis detection. AJR Am J Roentgenol. 2002. 179:911–916.
Article21. Kopp AF, Schroeder S, Kuettner A, Heuschmid M, Georg C, Ohnesorge B, et al. Coronary arteries: retrospectively ECG-gated multi-detector row CT angiography with selective optimization of the image reconstruction window. Radiology. 2001. 221:683–688.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Usefulness of Multidetector-row CT in the Evaluation of Reperfused Myocardial Infarction in a Rabbit Model
- Preoperative Radiologic Evaluation of Cholangiocarcinoma
- Cardiac MRI
- Combined Electrocardiography- and Respiratory-Triggered CT of the Lung to Reduce Respiratory Misregistration Artifacts between Imaging Slabs in Free-Breathing Children: Initial Experience
- Noncompaction of Ventricular Myocardium Involving the Right Ventricle
