Complete Visual Recovery after Mycotic Aneurysm Embolization Complicated by Cavernous Sinus Thrombophlebitis
- Affiliations
-
- 1Department of Ophthalmology, Kim's Eye Hospital, Konyang University College of Medicine, Seoul, Korea.
- 2Department of Neurology, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seongnam, Korea.
- 3Department of Neurosurgery, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seongnam, Korea.
- 4Department of Ophthalmology, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seongnam, Korea. hjm@snu.ac.kr
- KMID: 974330
- DOI: http://doi.org/10.3341/kjo.2010.24.5.322
Abstract
- A 62-year-old woman has been suffered from cavernous sinus thrombophlebitis which was confirmed by four-vessel angiography, orbit magnetic resonance imaging, and blood culture. Three weeks after recovery of cavernous sinus thrombophlebitis, right eye proptosis and complete third, fourth, and sixth cranial nerve palsies developed. Best-corrected visual acuity decreased to 20/70 in the right eye. Repeat magnetic resonance imaging demonstrated a 1.5-cm-sized mass in the right cavernous sinus, suspicious for mycotic aneurysm. Amphotericin B supplementation was begun and was followed by successful transarterial Guglielmi detachable coil embolization. Four months later, extraocular movement was normalized, and visual acuity improved to 20/25 in the right eye.
MeSH Terms
Figure
-
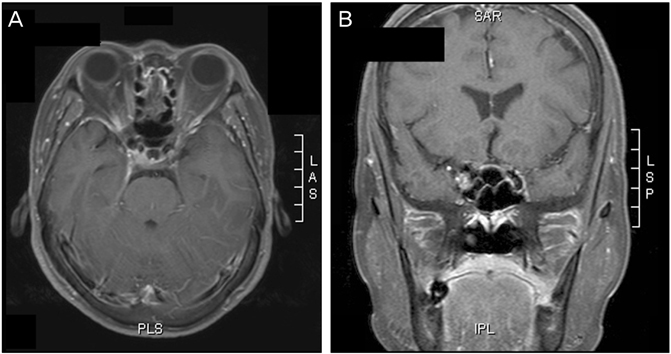
Fig. 1 Gadolinium-enhanced magnetic resonance imaging shows enhancement in the right cavernous sinus in the fat-suppressed T1-weighted axial image (A) and T1-weighted sagittal image (B).

Fig. 2 (A) Four-vessel angiography reveals that the cavernous sinus is not filled in the delayed views, and venous engorgement and stasis are shown (arrow). (B) Soft exudates and splinter hemorrhage are noted upon fundus examination. (C) Mycotic aneurysm is located at the cavernous sinus portion upon digital four-vessel angiography (arrow). (D) Guglielmi detachable coil embolization is performed successfully without the remaining aneurysm (arrow).
Cited by 1 articles
-
A Case of the Third, Fourth, and Sixth Nerve Palsy in a Patient with Cerebral Aspergillosis
Sung Soo Hwang, Soo Jung Lee
J Korean Ophthalmol Soc. 2015;56(3):471-476. doi: 10.3341/jkos.2015.56.3.471.
Reference
-
1. Hurst RW, Choi IS, Persky M, Kupersmith M. Mycotic aneurysms of the intracavernous carotid artery: a case report and review of the literature. Surg Neurol. 1992. 37:142–146.2. Wilson WR, Hawrych A, Olan W. Rapid development of bilateral internal carotid artery aneurysm from sphenoid sinus aspergillosis. Skull Base Surg. 1998. 8:211–214.3. Quisling SV, Mawn LA, Larson TC 3rd. Blindness associated with enlarging mycotic aneurysm after cavernous sinus thrombosis. Ophthalmology. 2003. 110:2036–2039.4. Koebbe CJ, Veznedaroglu E, Jabbour P, Rosenwasser RH. Endovascular management of intracranial aneurysms: current experience and future advances. Neurosurgery. 2006. 59:5 Suppl 3. S93–S102.5. Guglielmi G, Vinuela F, Dion J, Duckwiler G. Electrothrombosis of saccular aneurysms via endovascular approach. Part 2: Preliminary clinical experience. J Neurosurg. 1991. 75:8–14.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Endovascular Treatment of Large Mycotic Aneurysm in Cavernous Internal Carotid Artery : A Case Report
- Pseudoaneurysm of Internal Carotid Artery Secondaiy to the Cavernous Sinus Thrombophlebitis
- A Case of Cavernous Sinus Thrombophlebitis Secondary toAcute Isolated Sphenoid Sinusitis
- Oculomotor and Abducens Nerve Palsy Complicated by Cavernous Sinus Thrombophlebitis Resulting from Acute Sinusitis
- Clinical Aspect and Treatment of Intracranial Mycotic Aneurysm
