CT and US Findings of Multilocular Cystic Renal Cell Carcinoma
- Affiliations
-
- 1Department of Diagnostic Radiology, Chungnam National University School of Medicine, Taejeon, Korea. jckim@cnuh.co.kr
- KMID: 966481
- DOI: http://doi.org/10.3348/kjr.2000.1.2.104
Abstract
OBJECTIVE
Multilocular cystic renal cell carcinoma (MCRCC) is a recently described variety of renal cell carcinoma with characteristic pathologic and clinical features. The purpose of this study was to analyze the imaging findings of MCRCCs. MATERIALS AND METHODS: Ten adult patients with pathologically proven unilateral MCRCC who underwent renal US and CT were included in this study. The radiologic findings were retrospectively evaluated for cystic content, wall, septum, nodularity, calcification and solid portion by three radiologists who established a consensus. Imaging and postnephrectomy pathologic findings were compared. RESULTS: All patients were adults (six males and four females) and their ages ranged from 33 to 68 years (mean, 46). On US and CT images, all tumors appeared as well-defined multilocular cystic masses composed of serous or complicated fluid. In all patients, unenhanced CT scans revealed hypodense cystic portions, and in four tumors, due to the presence of hemorrhage or gelatinous fluid, some hyperdense areas were also noted. In no tumor was an expansile solid nodule seen in the thin septa, and in only one was there dystrophic calcification in a septum. Small areas of solid portion constituting less than 10% of the entire lesion were found in six of the ten tumors, and these areas were slightly enhanced on enhanced CT scans. In all patients, imaging and pathologic findings correlated closely. CONCLUSION: On US and CT images, MCRCC appeared as a well-defined multilocular cystic mass with serous, proteinaceous or hemorrhagic fluid, with no expansile solid nodules in the thin septa, and sometimes with small slightly enhanced solid areas. Where radiologic examinations demonstrate a cystic renal mass of this kind in adult males, MCRCC should be included in the differential diagnosis.
Keyword
MeSH Terms
Figure
-
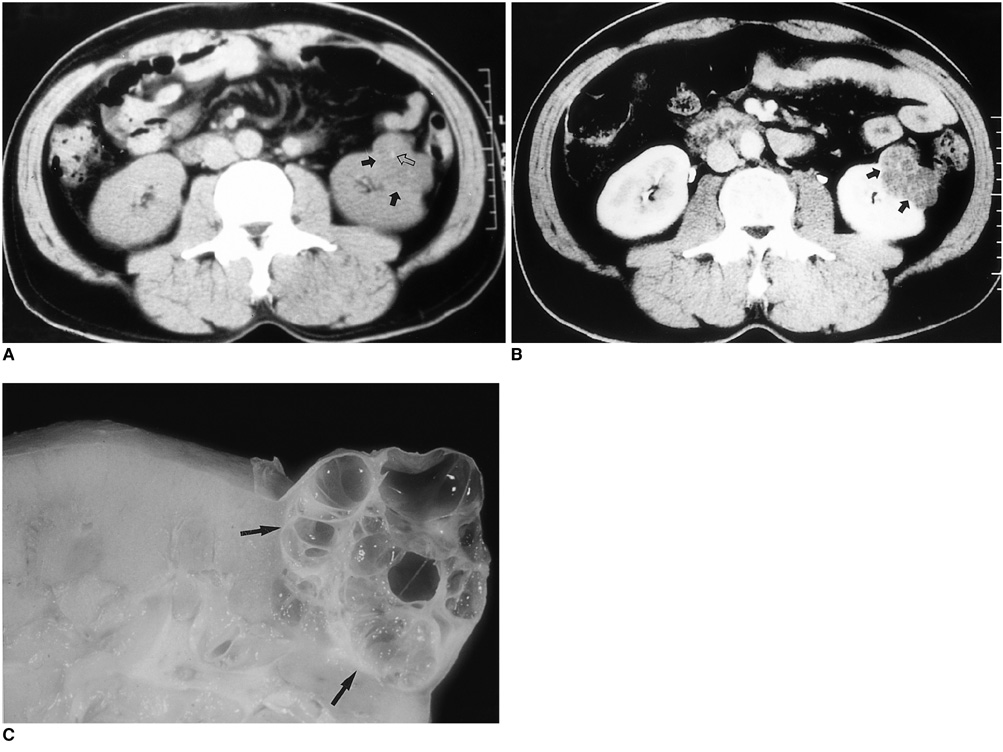
Fig. 1 A 41-year-old female with MCRCC in the left kidney (Case 2). A. Unenhanced CT scan shows a lobulated hypodense mass (solid arrows) in the antero-lateral aspect of the left kidney. Note a hyperdense spot (open arrow) in the mass, which pathologic examination showed to be an area of calcification. B. Enhanced CT scan shows a lobulated multiloculated cystic mass with multiple enhanced thin septa, nonenhanced fluid, and clear margin (arrows). The septa do not appear to have expanding nodules. C. Photograph of resected specimen reveals that the tumor is well-defined and divided into multiple locules by thin septa of less than one millimeter (arrows). The locules are filled with serous and gelatinous fluid, and the septa have no expanding solid nodules. Microscopic examination (not shown here) demonstrated that the septa consist of fibrous tissue with some collagenous portions, and the cyst walls are lined by a single layer of clear epithelial cells with grade 1 nuclear atypia.
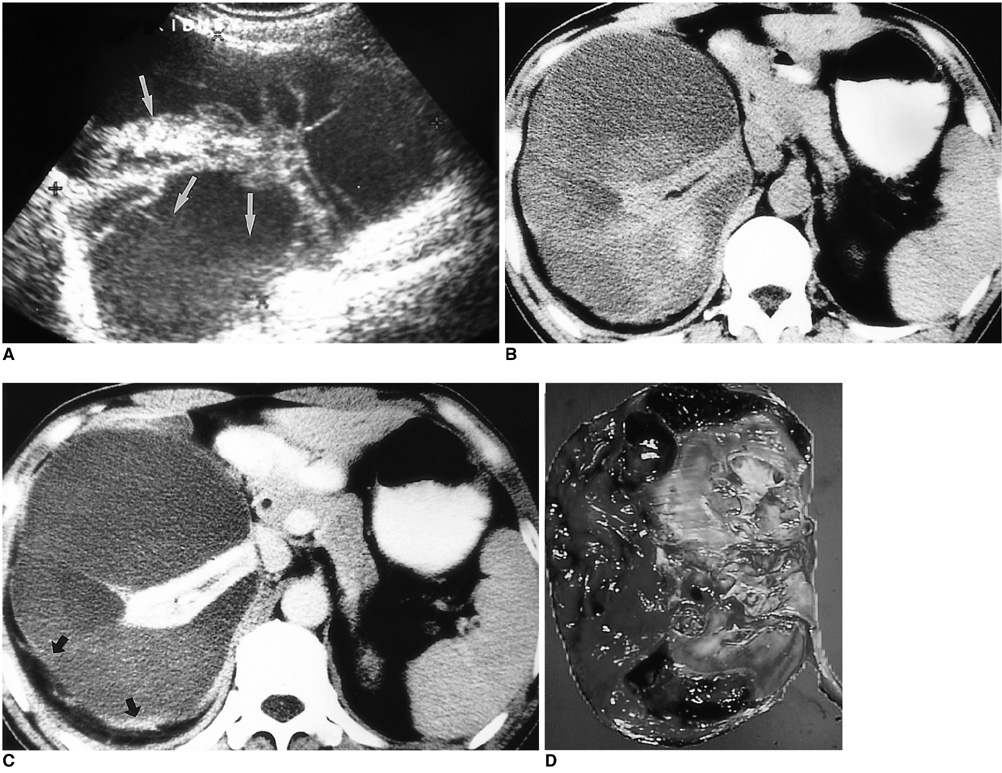
Fig. 2 A 38-year-old male with MCRCC in the right kidney (Case 5). A. Longitudinal US image shows a well-defined multilocular cystic mass in the right kidney separated by multiple echogenic thin septa. Note associated echogenic debris in the dependent portion of the locules, suggesting blood clots (arrows). B. Unenhanced CT scan shows a large well-defined multilocular cystic mass in the subcapsular portion of the right kidney, compressing the residual renal parenchyme medially and centrally. The variably sized cystic portions contain hypo-, iso-, or hyperdense fluid, depending on the presence of hemorrhage and/or proteinaceous fluid. C. Enhanced CT shows a multiloculated cystic mass with enhanced thin septa, nonenhanced fluid of varying density, and some enhanced solid portions (arrows). The thin septa do not show expanding nodules. D. Photograph of gross specimen reveals that the large subcapsular multiloculated cystic mass is composed of multiple thin septa without expanding solid nodules, a large amount of subcapsular hematoma and hemorrhagic fluid in the multicystic lesions, and a small number of solid portions constituting less than 10% of the entire lesion. Microscopic examination (not shown here) indicates that the cystic wall of the mass has extensive fibrosis, and aggregates of papillary clear cell carcinoma cells with abundant clear to eosinophilic granular cytoplasm.
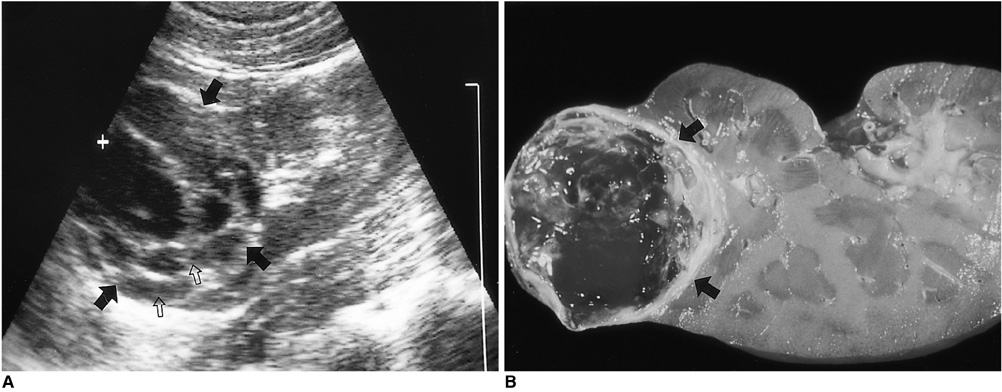
Fig. 3 A 43-year-old female with MCRCC in the right kidney (Case 6). A. Longitudinal US scan shows a well-defined multiloculated exophytic cystic mass with multiple thin septa in the upper pole of the right kidney (solid arrows). Note the associated echogenic debris in the dependent portions of the locules, suggesting blood clots (open arrows). B. Photograph of resected specimen reveals that the tumor is well encapsulated and divided into multiple locules by thin septa without expanding nodules (arrows). The cystic mass contains serous and hemorrhagic fluid.
Reference
-
1. Hartman DS, editor. The troublesome cystic renal mass. Proceedings of Uroradiology in Santa Fe' 97. 1997. 29–32.2. Murphy JB, Marshall FF. Renal cyst versus tumor: a continuing dilemma. J Urol. 1980. 123:566–569.3. Hartman DS, Davis CJ Jr, Johns T, Goldman SM. Cystic renal cell carcinoma. Urology. 1986. 283:145–153.4. Levy P, Helenon O, Merran S, et al. Cystic tumors of the kidney in adults: radiopathologic correlations. J Radiol. 1996. 80:121–133.5. Murad T, Komaiko W, Oyasu R, Bauer K. Multilocular cystic renal cell carcinoma. Am J Clin Pathol. 1991. 95:633–637.6. Eble JN, Bonsib SM. Extensively cystic renal neoplasms: cystic nephroma, cystic partially differentiated nephroblastoma, multilocular cystic renal cell carcinoma and cystic hamartoma of renal pelvis. Semin Diagn Radiol. 1998. 15:2–20.7. Yamashita Y, Miyazaki T, Ishii A, Watanabe O, Takahashi M. Multilocular cystic renal cell carcinoma presenting as a solid mass: radiologic evaluation. Abdom Imaging. 1995. 20:164–168.8. Feldeberg MAM, van Waes PFGM. Multilocular cystic renal cell carcinoma. AJR. 1982. 138:953–955.9. Levy P, Helenon O, Merran S, et al. Cystic tumors of the kidney in adults: radiohistopathologic correlations. J Radiol. 1999. 80:121–133.10. Bielsa O, Lloreta J, Gelabert-Mas A. Cystic renal cell carcinoma: pathological features, survival and implications for treatment. Br J Urol. 1998. 82:16–20.11. Ooi GC, Sagar G, Lynch D, Arkell DG, Ryan PG. Cystic renal cell carcinoma: radiological features and clinico-pathological correlation. Clin Radiol. 1996. 51:791–796.12. Robinson GL. Perlman's tumor of the kidney. Br J Surg. 1957. 44:620–623.13. Weiss SG 2nd, Hafez RG, Uehling DT. Multilocular cystic renal cell carcinoma: implications for nephron sparing surgery. Urology. 1998. 51:635–637.14. Madewell JE, Goldman SM, Davis CJ Jr, Hartman DS, Feigin DS, Lichtenstein JE. Multilocular cystic nephroma: a radiographic-pathologic correlation of 58 patients. Radiology. 1983. 146:309–321.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Multilocular Cystic Renal Cell Carcinoma
- CT and US Findings of the Multilocular Cystic Renal Cell Carcinoma
- A case of multilocular cystic renal cell carcinoma mistaken for multilocular renal cyst
- Multilocular Cystic Renal Cell Carcinoma: A case report
- Multilocular Cystic Renal Cell Carcinoma Treated with Wedge Resection
