Two Cases of Corneal Ulcer due to Methicillin-Resistant Staphylococcus aureus in High Risk Groups
- Affiliations
-
- 1Department of Ophthalmology and Visual Science, The Catholic University of Korea School of Medicine, Seoul, Korea. mskim@catholic.ac.kr
- 2HanGil Eye Hospital, Incheon, Korea.
- KMID: 949063
- DOI: http://doi.org/10.3341/kjo.2010.24.4.240
Abstract
- Considering the popular use of antibiotic-containing eyedrops in Korea, it is important to know the emerging antibiotic-resistant strains of bacteria before treating infectious eye diseases. This is especially important in high-risk groups because of the high incidence of resistant infections and the subsequent treatment requirements. We report two cases of methicillin-resistant Staphylococcus aureus (MRSA) corneal ulcers in high-risk groups. The first case involved a patient who had keratitis after using antibiotic- and steroid-containing eyedrops to treat a corneal opacity that developed after repeated penetrating keratoplasty. The second case involved a patient who used antibiotic-containing eyedrops and a topical lubricant on a regular basis for >1 month to treat exposure keratitis due to lagophthalmos. The second patient's problems, which included a persistent superficial infiltration, developed after brain tumor surgery. Both cases showed MRSA on corneal culture, and the corneal ulcers improved in both patients after the application of vancomycin-containing eyedrops. In conclusion, MRSA infection should be considered in corneal ulcers that have a round shape, mild superficial infiltration, and slow progression, especially in high-risk groups. This report includes descriptions of the characteristic features, antibiotic sensitivities, prevention, and successful treatment with vancomycin-containing eyedrops for MRSA corneal ulcers.
MeSH Terms
-
Cornea/*microbiology/pathology
Corneal Ulcer/diagnosis/*microbiology
Diagnosis, Differential
Eye Infections, Bacterial/diagnosis/*microbiology
Female
Follow-Up Studies
Humans
Male
Methicillin-Resistant Staphylococcus aureus/*isolation & purification
Middle Aged
Staphylococcal Infections/diagnosis/*microbiology
Figure
-
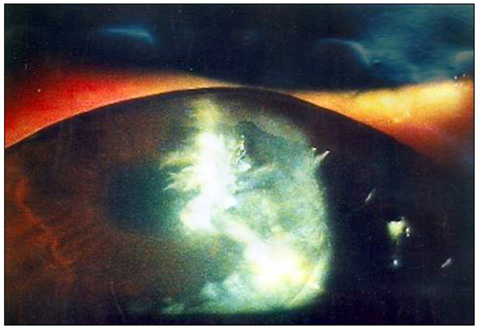
Fig. 1 Corneal ulcer after penetrating keratoplasty and persistent use of levofloxacin and steroid eyedrops (case 1). On slit lamp examination, a 4×3 mm round corneal opacity with a corneal epithelial defect associated with mild superficial stromal infiltration was found at the 2 to 3 o/c area around the penetrating keratoplasty stitch. Corneal edema was also noted.
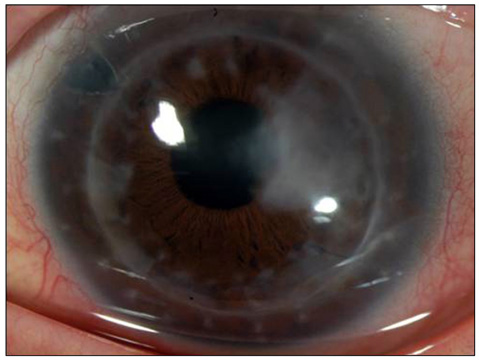
Fig. 2 Recovery of the corneal ulcer after 2 months of vancomycin eyedrops (case 1). The corneal epithelial defect with infiltration disappeared, but the corneal opacity remained. The corneal edema resolved.
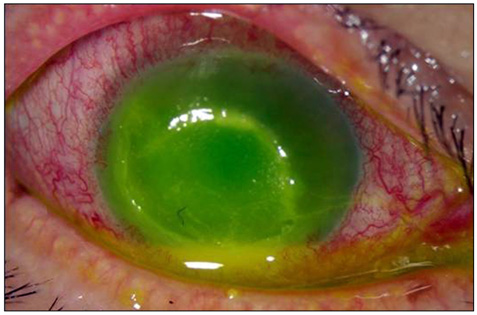
Fig. 3 Corneal ulcer after persistent use of levofloxacin eyedrops and lubricant for exposure keratitis (case 2). On slit lamp examination, an 8×8 mm round corneal ulcer with superficial stromal infiltration was found. The anterior chamber contained a 1.5 mm hypopyon associated with ciliary injection.
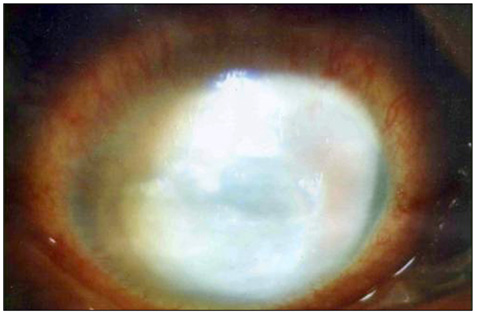
Fig. 4 (A) Gram stain of the eye discharge showed gram-positive spherical, paired bacteria. (B) The agar plate culture of the eye discharge showed large yellow colonies which were Staphylococcus aureus and small white colonies which were Staphylococcus epidermidis (case 2).
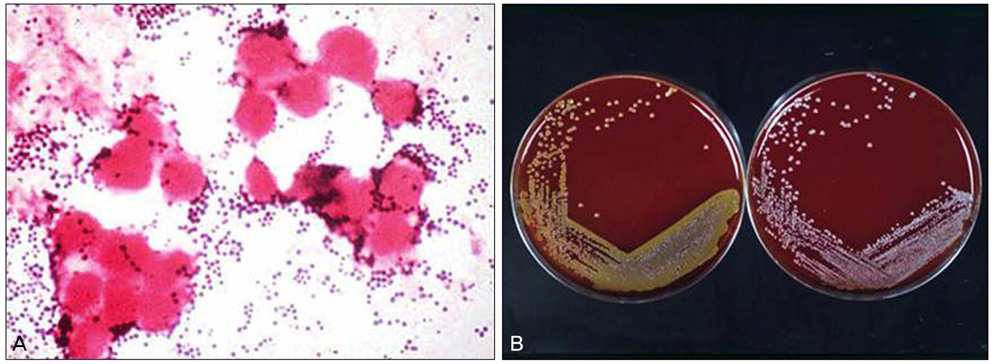
Fig. 5 Recovery of the corneal ulcer after 5 days of vancomycin eyedrops (case 2). The corneal ulcer decreased in size to 5×4 mm. The superficial infiltration and hypopyon also decreased in size.
Reference
-
1. Brumfitt W, Hamilton-Miller J. Methicillin-resistant Staphylococcus aureus. N Engl J Med. 1989. 320:1188–1196.2. Kirby WM. Extraction of a highly potent penicillin inactivator from penicillin resistant staphylococci. Science. 1944. 99:452–453.3. Rolinson GN, Stevens S, Batchelor FR, et al. Bacteriological studies on a new penicillin-BRL. 1241. Lancet. 1960. 2:564–567.4. Jevons MP. "Celbenin"-resistant Staphylococci. Br Med J. 1961. 1:124–125.5. Knox R. "Celbenin"-resistant Staphylococci. Br Med J. 1961. 1:126.6. Sahm DF, Marsilio MK, Piazza G. Antimicrobial resistance in key bloodstream bacterial isolates: electronic surveillance with the Surveillance Network Database: USA. Clin Infect Dis. 1999. 29:259–263.7. Diekema DJ, Pfaller MA, Schmitz FJ, et al. Survey of infections due to Staphylococcus species: frequency of occurrence and antimicrobial susceptibility of isolates collected in the United States, Canada, Latin America, Europe, and the Western Pacific region for the SENTRY Antimicrobial Surveillance Program, 1997-1999. Clin Infect Dis. 2001. 32:Suppl 2. S114–S132.8. Sotozono C, Inagaki K, Fujita A, et al. Methicillin-resistant Staphylococcus aureus and methicillin-resistant Staphylococcus epidermidis infections in the cornea. Cornea. 2002. 21:S94–S101.9. Kim IS, Shin YM, Kim SJ, et al. Comparison of antimicrobial efficacy of topical antibiotics in rabbit keratitis model with ciprofloxacin, methicillin-resistant Staphylococcus aureus. J Korean Ophthalmol Soc. 2000. 41:807–814.10. Insler MS, Fish LA, Silbernagel J, et al. Successful treatment of methicillin-resistant Staphylococcus aureus Keratitis with topical ciprofloxacin. Ophthalmology. 1991. 98:1690–1692.11. Snyder ME, Katz HR. Ciprofloxacin-resistant bacterial keratitis. Am J Ophthalmol. 1992. 114:336–338.12. Harbarth S, Francois P, Shrenzel J, et al. Community-associated methicillin-resistant Staphylococcus aureus, Switzerland. Emerg Infect Dis. 2005. 11:962–965.13. Charlebois ED, Bangsberg DR, Moss NJ, et al. Population-based community prevalence of methicillin-resistant Staphylococcus aureus in the urban poor of San Francisco. Clin Infect Dis. 2002. 34:425–433.14. Pan ES, Diep BA, Charlebois ED, et al. Population dynamics of nasal strains of methicillin-resistant Staphylococcus aureus and their relation to community-associated disease activity. J Infect Dis. 2005. 192:811–818.15. Blomquist PH. Methicillin-resistant Staphylococcus aureus infections of the eye and orbit (an American Ophthalmological Society thesis). Trans Am Ophthalmol Soc. 2006. 104:322–345.16. Maple PA, Hamilton-Miller JM, Brumfitt W. World-wide antibiotic resistance in methicillin-resistant Staphylococcus aureus. Lancet. 1989. 1:537–540.17. Brennen C, Muder RR. Conjunctivitis associated with methicillin-resistant Staphylococcus aureus in a long-term-care facility. Am J Med. 1990. 88:14N–17N.18. Mulligan ME, Murray-Leisure KA, Ribner BS, et al. Methicillin-resistant Staphylococcus aureus: a consensus review of the microbiology, pathogenesis, and epidemiology with implications for prevention and management. Am J Med. 1993. 94:313–328.19. Herwaldt LA. Control of methicillin-resistant Staphylococcus aureus in the hospital setting. Am J Med. 1999. 106:11S–18S.20. Pittet D, Hugonnet S, Harbarth S, et al. Effectiveness of a hospital-wide programme to improve compliance with hand hygiene: Infection Control Programme. Lancet. 2000. 356:1307–1312.21. Fleischer AB, Hoover DL, Khan JA, et al. Topical vancomycin formulation for methicillin-resistant Staphylococcus epidermidis blepharoconjunctivitis. Am J Ophthalmol. 1986. 101:283–287.22. Forster W, Becker K, Hungermann D, Busse H. Methicillin-resistant Staphylococcus aureus keratitis after excimer laser photorefractive keratectomy 1. J Cataract Refract Surg. 2002. 28:722–724.23. Goodman DF, Gottsch JD. Methicillin-resistant Staphylococcus epidermidis keratitis treated with vancomycin. Arch Ophthalmol. 1988. 106:1570–1571.24. Khan JA, Hoover D, Ide CH. Methicillin-resistant Staphylococcus epidermidis blepharitis. Am J Ophthalmol. 1984. 98:562–565.25. Shanmuganathan VA, Armstrong M, Buller A, Tullo AB. External ocular infections due to methicillin-resistant Staphylococcus aureus (MRSA). Eye (Lond). 2005. 19:284–291.26. Rutar T, Chambers HF, Crawford JB, et al. Ophthalmic manifestations of infections caused by the USA300 clone of community-associated methicillin-resistant Staphylococcus aureus. Ophthalmology. 2006. 113:1455–1462.27. Kato T, Hayasaka S. Methicillin-resistant Staphylococcus aureus and methicillin-resistant coagulase-negative staphylococci from conjunctivas of preoperative patients. Jpn J Ophthalmol. 1998. 42:461–465.28. Mitsuda T, Arai K, Fujita S, Yokota S. Epidemiological analysis of strains of methicillin-resistant Staphylococcus aureus (MRSA) infection in the nursery: prognosis of MRSA carrier infants. J Hosp Infect. 1995. 31:123–134.29. Cooper BS, Stone SP, Kibbler CC, et al. Isolation measures in the hospital management of methicillin resistant Staphylococcus aureus (MRSA): systematic review of the literature. BMJ. 2004. 329:533.30. Boyce JM, Potter-Bynoe G, Chenevert C, King T. Environmental contamination due to methicillin-resistant Staphylococcus aureus: possible infection control implications. Infect Control Hosp Epidemiol. 1997. 18:622–627.31. Devine J, Cooke RP, Wright EP. Is methicillin-resistant Staphylococcus aureus (MRSA) contamination of ward-based computer terminals a surrogate marker for nosocomial MRSA transmission and handwashing compliance? J Hosp Infect. 2001. 48:72–75.32. Layton MC, Perez M, Heald P, Patterson JE. An outbreak of mupirocin-resistant Staphylococcus aureus on a dermatology ward associated with an environmental reservoir. Infect Control Hosp Epidemiol. 1993. 14:369–375.33. Dietze B, Rath A, Wendt C, Martiny H. Survival of MRSA on sterile goods packaging. J Hosp Infect. 2001. 49:255–261.34. Muto CA, Jernigan JA, Ostrowsky BE, et al. SHEA guideline for preventing nosocomial transmission of multidrug-resistant strains of Staphylococcus aureus and enterococcus. Infect Control Hosp Epidemiol. 2003. 24:362–386.35. Suh Y, Shin EM, Hahn TW. Corneal ulcer and chronic conjunctivitis due to ofloxacin-resistant MRSA. J Korean Ophthalmol Soc. 2002. 43:419–423.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Detection of Multidrug Resistant Patterns and Associated - genes of Methicillin Resistant Staphylococcus aureus ( MRSA ) Isolated from Clinical Specimens
- A statistical analysis of methicillin-resistant staphylococcus aureus
- A case of multiple furunculosis caused by methicillin-resistant staphylococcs aureus
- Corneal Ulcer and Chronic Conjunctivitis Due to Ofloxacin-resistant MRSA
- Community-associated methicillin-resistant Staphylococcus aureus (CA-MRSA)
