Korean J Gastroenterol.
2010 Sep;56(3):205-208. 10.4166/kjg.2010.56.3.205.
Hemobilia as the Initial Manifestation of Cholangiocarcinoma in a Patient with Choledochoduodenostomy
- Affiliations
-
- 1Department of Internal Medicine, Pusan National University School of Medicine, Busan, Korea. doc0224@chol.com
- KMID: 948784
- DOI: http://doi.org/10.4166/kjg.2010.56.3.205
Abstract
- Hemobilia occurs when injury or disease causes communication between intrahepatic blood vessels and the intrahepatic or extrahepatic biliary system. The causes of hemobilia include trauma, gallstone disease, vascular malformation, inflammation, and biliary or hepatic tumors. Hemobilia could be diagnosed by endoscopy, hepatic angiography, computed tomography, and ultrasonogram. Patients with hemobilia may present with biliary colic, obstructive jaundice and gastrointestinal bleeding. Extrahepatic cholangiocarcinoma usually presents with obstructive jaundice and is one of the unusual cause of hemobilia. We, herein, report a case of hemobilia caused by cholangiocarcinoma in a 69-year-old woman. She had the past history of lung cancer and choledochoduodenostomy due to gallstone. Esophagogastroduodenoscopy revealed a blood clot protruding from the choledochoduodenostomy site and the ulcerative mass in the common bile duct. Pathologic examination of the ulcerative mass was compatible with those of cholangiocarcinoma.
MeSH Terms
Figure
-
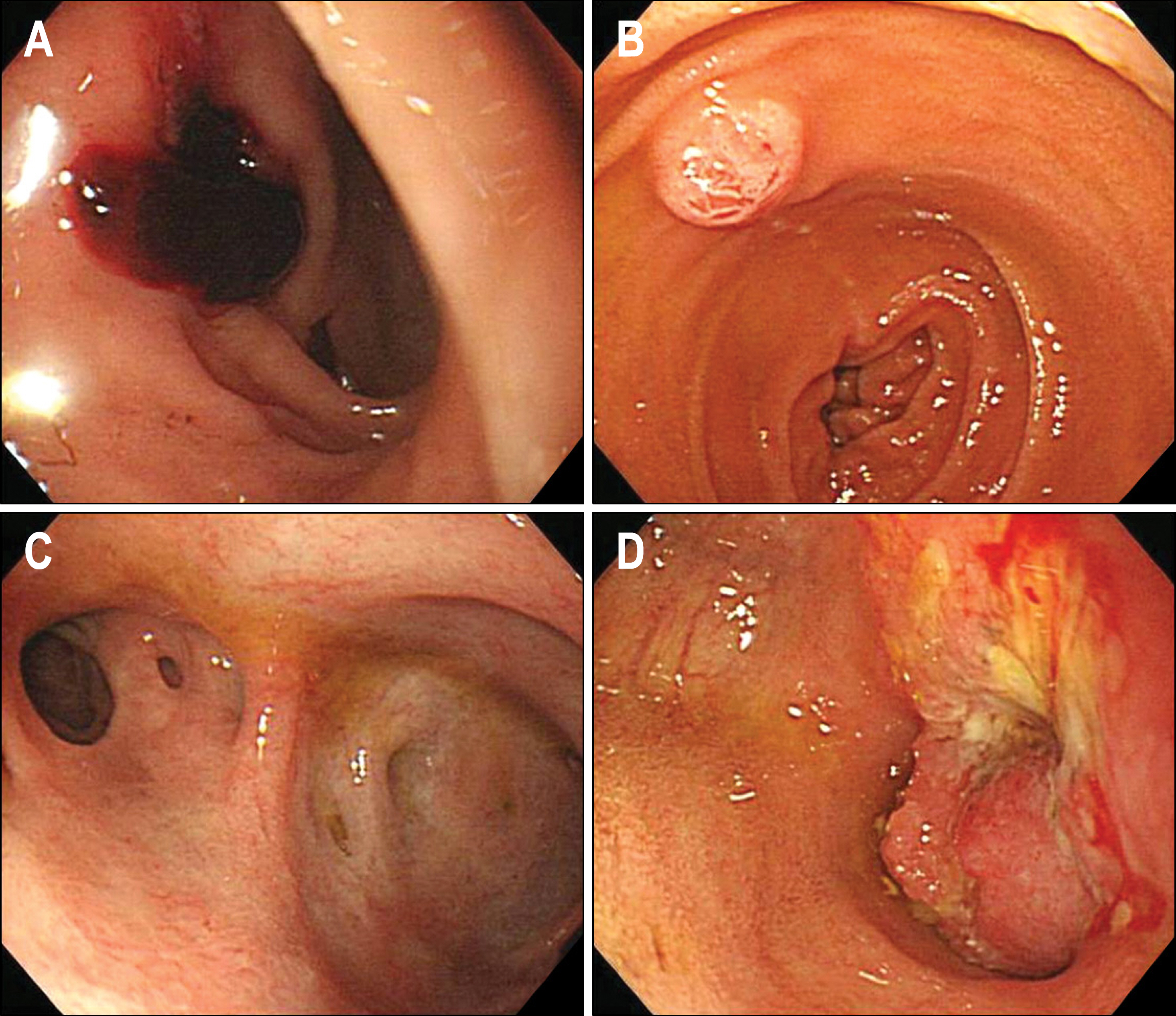
Fig. 1. Esophagogastroduodenoscopy revealed (A) a blood clots protruding from choledochoduodenostomy site, (B) normal Ampulla of Vater, (C) no abnormal lesion in intrahepatic bile duct and (D) a ulcerative mass in the distal common bile duct.
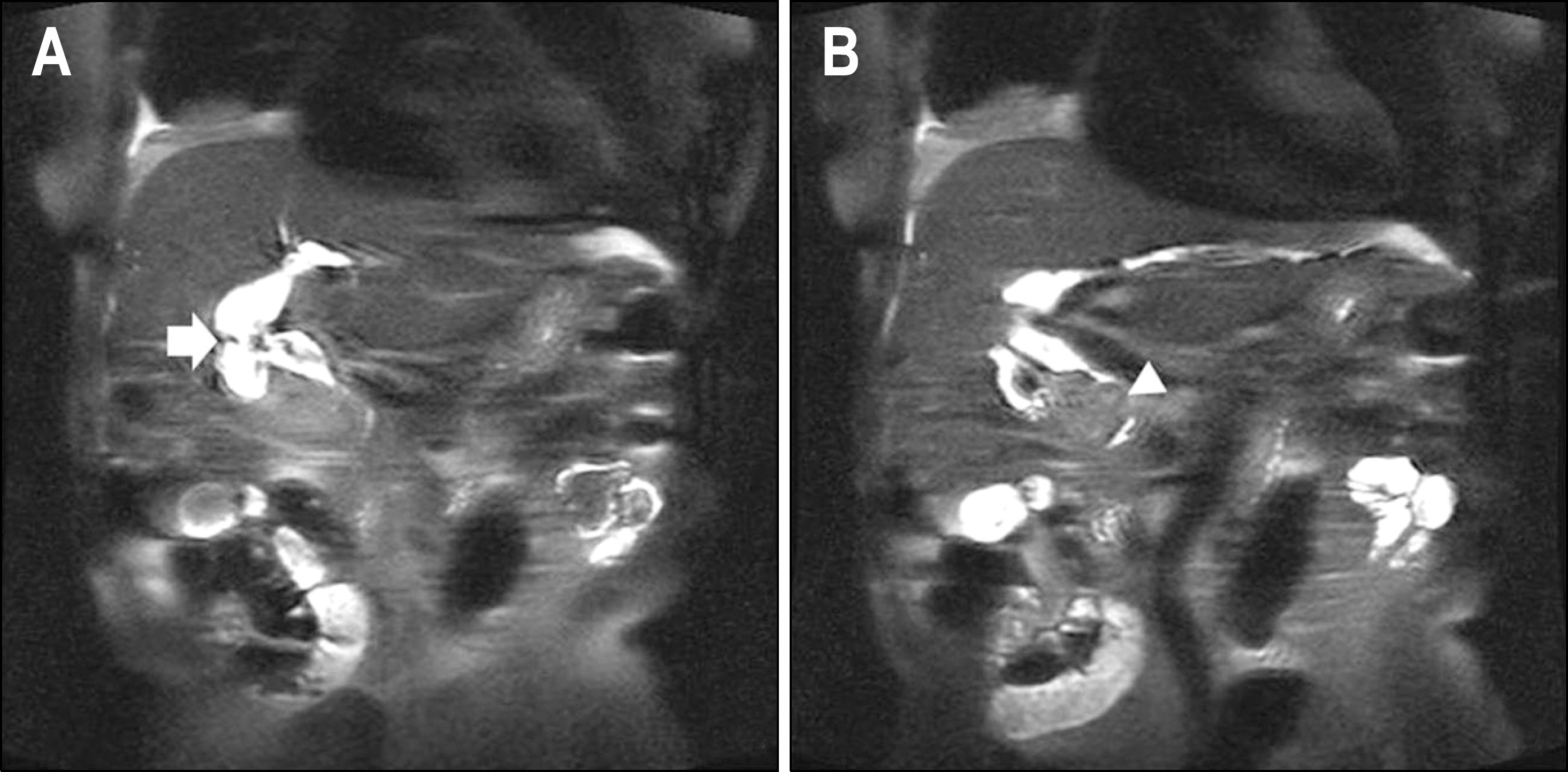
Fig. 2. Magnetic resonance chol-angiopancreatography revealed (A) choledochoduodenostomy site at perihilar area (arrow) and (B) ec-centric narrowing of distal common bile duct due to a mass (arrow head).
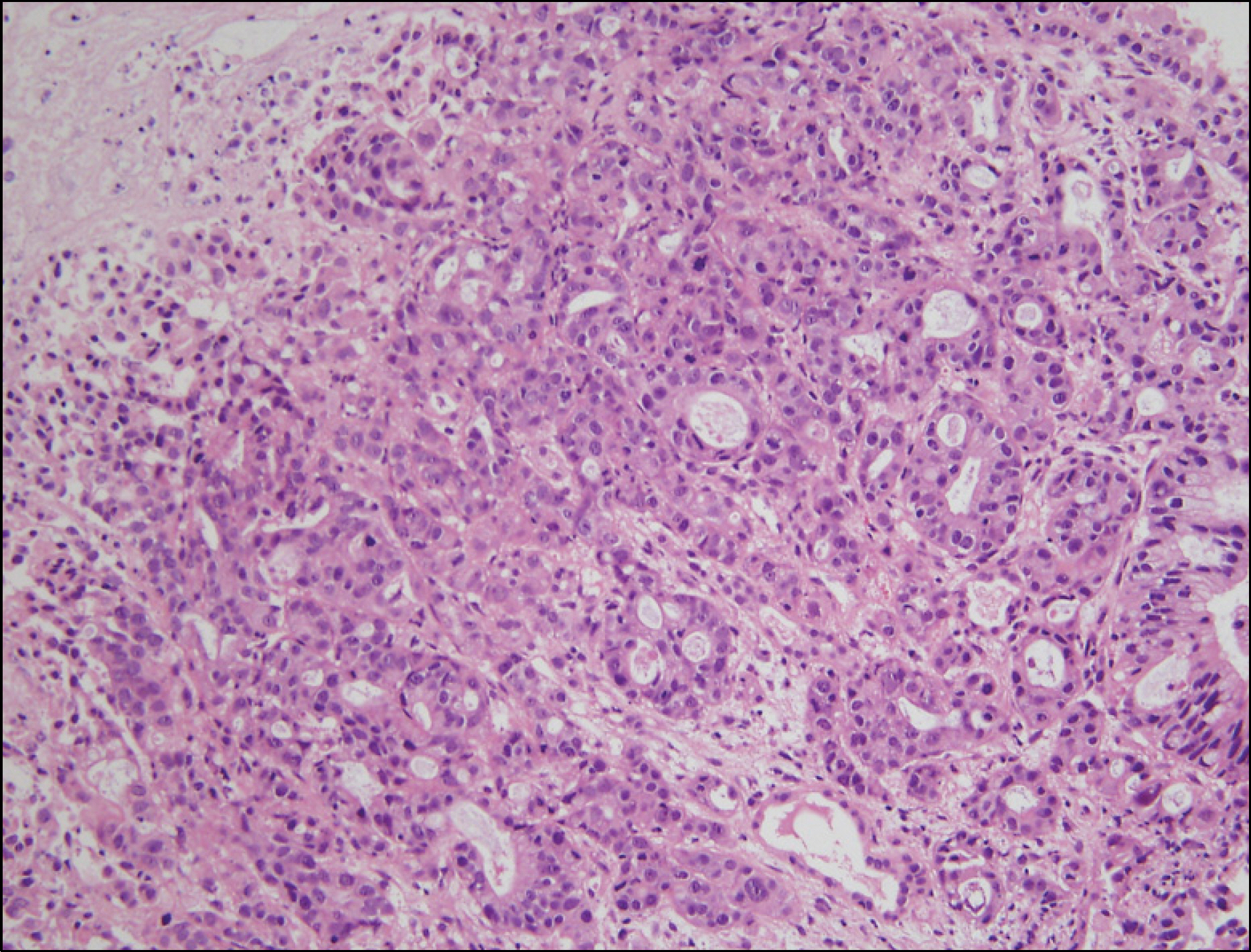
Fig. 3. Pathologic examination of the ulcerative mass in distal common bile duct revealed the irregular glandular structures with tumor cells, compatible with those of cholangiocarcinoma. (H&E, ×200).
Reference
-
1. Bloechle C, Izbicki JR, Rashed MY, et al. Hemobilia: pre-sentation, diagnosis, and management. Am J Gastroenterol. 1994; 89:1537–1540.2. Green MH, Duell RM, Johnson CD, Jamieson NV. Haemobilia. Br J Surg. 2001; 88:773–786.
Article3. Goodnight JE Jr, Blaisdell FW. Hemobilia. Surg Clin North Am. 1981; 61:973–979.
Article4. Sandblom P. Iatrogenic hemobilia. Am J Surg. 1986; 151:754–758.
Article5. Murata K, Oohashi Y, Takase K, Nakano T, Tameda Y. A case of hemobilia after percutaneous liver biopsy treated by transcatheter arterial embolization with Histoacryl. Am J Gastroenterol. 1996; 91:160.6. Savader SJ, Trerotola SO, Merine DS, Venbrux AC, Osterman FA. Hemobilia after percutaneous transhepatic biliary drainage: treatment with transcatheter embolotherapy. J Vasc Interv Radiol. 1992; 3:345–352.
Article7. Ribeiro A, Williams H, May G, Fulmer JT, Spivey JR. Hemobilia due to hepatic artery pseudoaneurysm thirteen months after laparoscopic cholecystectomy. J Clin Gastroenterol. 1998; 26:50–53.
Article8. Willner IR, El-Sakr R, Werkman RF, Taylor WZ, Riely CA. A fistula from the portal vein to the bile duct: an unusual complication of transjugular intrahepatic portosystemic shunt. Am J Gastroenterol. 1998; 93:1952–1955.
Article9. Parks RW, Chrysos E, Diamond T. Management of liver trauma. Br J Surg. 1999; 86:1121–1135.
Article10. Ellington RT, Seidel RH, Burdick JS, Peterson WL, Harford WV. Acalculous cholecystitis presenting as hemobilia and jaundice. Gastrointest Endosc. 2000; 51:218–220.
Article11. Tan PS, Teo EK, Fock KM, Ang TL, Tan JY, Tan AG. Massive obscure-overt upper gastrointestinal bleeding secondary to hemobilia. Endoscopy. 2009; 41(suppl 2):E294–E295.
Article12. Nakeeb A, Pitt HA, Sohn TA, et al. Cholangiocarcinoma. A spectrum of intrahepatic, perihilar, and distal tumors. Ann Surg. 1996; 224:463–473.13. Sandblom P, Mirkovitch V. Minor hemobilia. Clinical significance and pathophysiological background. Ann Surg. 1979; 190:254–264.
Article14. Sandblom P. Hemobilia (biliary tract hemorrhage): history, pathology, diagnosis, treatment. 1st ed.Springfield, Ⅲ.: Thomas;1972.15. Yoshida J, Donahue PE, Nyhus LM. Hemobilia: review of recent experience with a worldwide problem. Am J Gastroenterol. 1987; 82:448–453.16. Merrell SW, Schneider PD. Hemobilia–evolution of current diagnosis and treatment. West J Med. 1991; 155:621–625.17. Lugagne PM, Lacaine F, Bonnel D, Ligory C, Huguier M. Bilioportal fistula as a complication of choledochoduodenostomy. Surgery. 1988; 103:125–129.18. Khan SA, Davidson BR, Goldin R, et al. Guidelines for the diagnosis and treatment of cholangiocarcinoma: consensus document. Gut. 2002; 51(suppl 6):VI1–9.
Article19. Lee SY, Yoon SG, Lee NS, et al. A case of hemobilia developing obstructive jaundice by blood clots in a patient with cholangiocarcinoma. Korean J Gastrointest Endosc. 1993; 13:419–423.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Hemobilia Developed in a Hepatic Artery Aneurysm after Biliary Stenting
- A Case of Hemobilia Developing Obstructive Jaundice by Blood Clots in a Patient with Cholangiocarcinoma
- Successful Treatment of an Iatrogenic Hepatic Arteriobiliary Fistula with an Endobiliary Covered Stent Graft: A Case Report
- A Case of Hemobilia Caused by Clonorchiasis
- Metal Stents for the Management of Massive Hemobilia in Patients with Hilum-Involving Cholangiocarcinoma Receiving MultiRegimen Chemotherapy
