The Usefulness of Fast-Spin-Echo T2-Weighted MR Imaging in Nutcracker Syndrome: a Case Report
- Affiliations
-
- 1Department of Radiology, Yuan's General Hospital, Kaohsiung 80249, Taiwan. jjychen@gmail.com
- 2National Yang-Ming University, School of Medicine, Taipei 112, Taiwan.
- 3Department of Internal Medicine, Division of Gastroenterology, Yuan's General Hospital, Kaohsiung 80249, Taiwan.
- 4Department of Internal Medicine, Division of Nephrology, Yuan's General Hospital, Kaohsiung 80249, Taiwan.
- 5Department of Radiology, Kaohsiung Veterans General Hospital, Kaohsiung 81362, Taiwan.
- KMID: 946280
- DOI: http://doi.org/10.3348/kjr.2010.11.3.373
Abstract
- Nutcracker syndrome occurs when the left renal vein (LRV) is compressed between the superior mesenteric artery and the aorta, and this syndrome is often characterized by venous hypertension and related pathologies. However, invasive studies such as phlebography and measuring the reno-caval pressure gradient should be performed to identify venous hypertension. Here we present a case of Nutcracker syndrome where the LRV and intra-renal varicosities appeared homogeneously hyperintense on magnetic resonance (MR) fast-spin-echo T2-weighted imaging, which suggested markedly stagnant intravenous blood flow and the presence of venous hypertension. The patient was diagnosed and treated without obtaining the reno-caval pressure gradient. The discomfort of the patient lessened after treatment. Furthermore, on follow-up evaluation, the LRV displayed a signal void, and this was suggestive of a restoration of the normal LRV flow and a decrease in LRV pressure.
Keyword
MeSH Terms
Figure
-
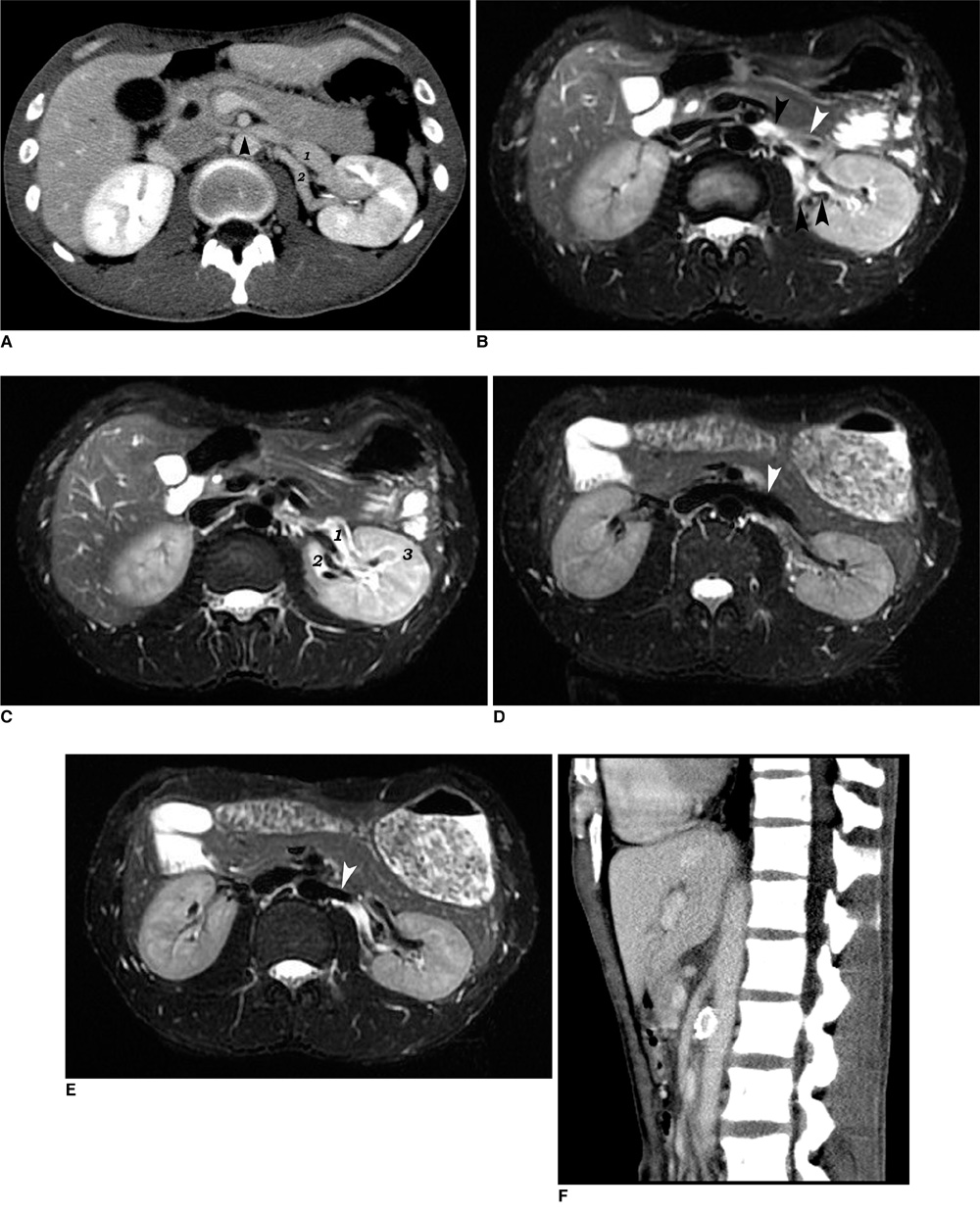
Fig. 1 Nutcracker syndrome in 24-year-old man. A. Contrast-enhanced CT scan before treatment. 1 = distended anterior left renal vein, 2 = distended posterior left renal vein. Common left renal vein between superior mesenteric artery and aorta is compressed (arrowhead), and left kidney is of relatively lower density than that of right kidney. B. MR fast-spin-echo T2WI before treatment revealed hyperintense left renal veins (black arrowheads). Note that vascular structures (vena cava, portal vein, superior mesenteric artery, aorta and distal common left renal vein) without flow stagnation appear as signaling voids. There was dark-grey area in anterior left renal vein (white arrowhead), which was flow artifact. C. MR fast-spin-echo T2WI one slice cranial to A. 1 = anterior left renal vein, 2 = posterior left renal vein, 3 = intra-renal collateral vein. Note that left kidney appears slightly hyperintense compared to that of right kidney, suggesting left renal swelling secondary to venous hypertension. D. MR fast-spin-echo T2WI performed one month after inserting endoprosthesis. Confluence of anterior and posterior left renal veins is shown (white arrowhead). All visible vascular structures appear as signaling voids. Note that signaling intensities are not different between right and left kidneys. E. MR fast-spin-echo T2WI one slice cranial to D. Anterior left renal vein gave dark signal. Posterior left renal vein remained bright, and this is probably due to external compression by left renal artery (white arrowhead), which may have caused intravenous flow stagnation. F. Contrast enhanced CT scan in sagittal plane after left renal vein stent insertion. Note sharp branching angle of superior mesenteric artery from aorta. High density ring in aorto-mesenteric space is cross-section of stent.
Reference
-
1. de Schepper A. "Nutcracker" phenomenon of the renal vein and venous pathology of the left kidney. J Belge Radiol. 1972. 55:507–511. [Dutch].2. Hohenfellner M, Steinbach F, Schultz-Lampel D, Schantzen W, Walter K, Cramer BM, et al. The nutcracker syndrome: new aspects of pathophysiology, diagnosis and treatment. J Urol. 1991. 146:685–688.3. Takebayashi S, Ueki T, Ikeda N, Fujikawa A. Diagnosis of the nutcracker syndrome with color Doppler sonography: correlation with flow patterns on retrograde left renal venography. AJR Am J Roentgenol. 1999. 172:39–43.4. Buschi AJ, Harrison RB, Norman A, Brenbridge AG, Williamson BR, Gentry RR, et al. Distended left renal vein: CT/sonographic normal variant. AJR Am J Roentgenol. 1980. 135:339–342.5. Kim SH, Cho SW, Kim HD, Chung JW, Park JH, Han MC. Nutcracker syndrome: diagnosis with Doppler US. Radiology. 1996. 198:93–97.6. Nishimura Y, Fushiki M, Yoshida M, Nakamura K, Imai M, Ono T, et al. Left renal vein hypertension in patients with left renal bleeding of unknown origin. Radiology. 1986. 160:663–667.7. Bluemke DA, Wolf RL, Tani I, Tachiki S, McVeigh ER, Zerhouni EA. Extremity veins: evaluation with fast-spin-echo MR venography. Radiology. 1997. 204:562–565.8. Hashemi RH. Hashemi RH, Bradley WG, Lisanti CJ, editors. Flow phenomena. MRI: the basics. 2004. 2nd ed. Philadelphia: Lippincott Williams & Wilkins;293–309.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Diagnosis of Meniscal Tear of the Knee Using Proton-weighted Fast Spin-Echo MR Imaging: Can be an Alternative to Conventional Spin-Echo Imaging?
- Meniscal Tears of the Knee: Diagnosis with Fast Spin-Echo MR Imaging and Role of Gadolinium-Enhancement
- Usefulness of CISS Technique in the MR Imaging Diagnosis of Intraocular Lesions
- Usefulness of Fluid Attenuated Inve rsion Re c overy(FLAIR) Image
- Fast FLAIR MR Imaging Finidngs of Cerebral Infarction: Comparison with T2-Weighted Spin Echo Imaging
