Trichilemmal Carcinoma of the Upper Eyelid: A Case Report
- Affiliations
-
- 1Department of Ophthalmology, Hanyang University School of Medicine, Seoul, Korea.
- 2Department of Pathology, Hanyang University Guri Hospital, Hanyang University School of Medicine, Guri, Korea.
- 3Department of Ophthalmology, Hanyang University Guri Hospital, Hanyang University School of Medicine, Guri, Korea. lyjot@hanyang.ac.kr
- KMID: 754768
- DOI: http://doi.org/10.3341/kjo.2009.23.4.301
Abstract
- We report a very rare case of trichilemmal carcinoma (TLC) involving the upper eyelid. To the best of our knowledge, this is the first report of trichilemmal carcinoma of the upper eyelid in Korea. A 51-year-old man presented to our hospital complaining of a bloody discharge from his left upper eyelid. He had a soft and lobulated mass on the palpebral conjunctiva. An incisional biopsy revealed trabecular growth of tumor cells with clear cytoplasm, prominent nucleoli, frequent mitoses, and foci of trichilemmal keratinization. Immunohistochemically, the lesion was positive for p53 and negative for CD 34. A diagnosis of TLC was made, and total excision of the mass and reconstruction of the eyelid were performed. Trichilemmal carcinoma is a rare malignant tumor, though it appears to be an indolent neoplasm with no metastatic potential. The treatment of choice for trichilemmal carcinoma of the eyelid is complete excision with tumor-free margins due to the locally invasive nature of the lesion.
Keyword
MeSH Terms
Figure
-
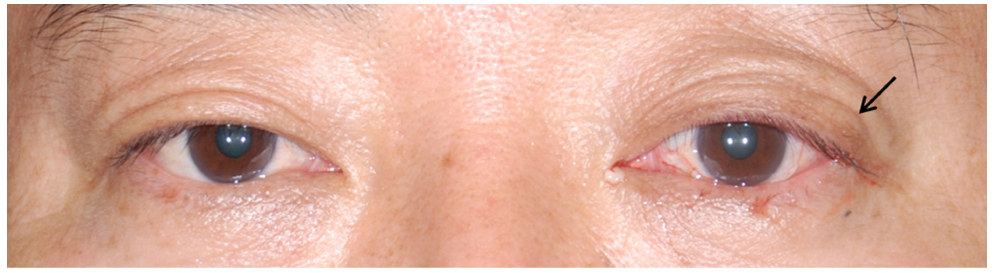
Fig. 1 The patient had a swelling of the upper eyelid and a palpable, nontender, movable mass on the left eyelid.
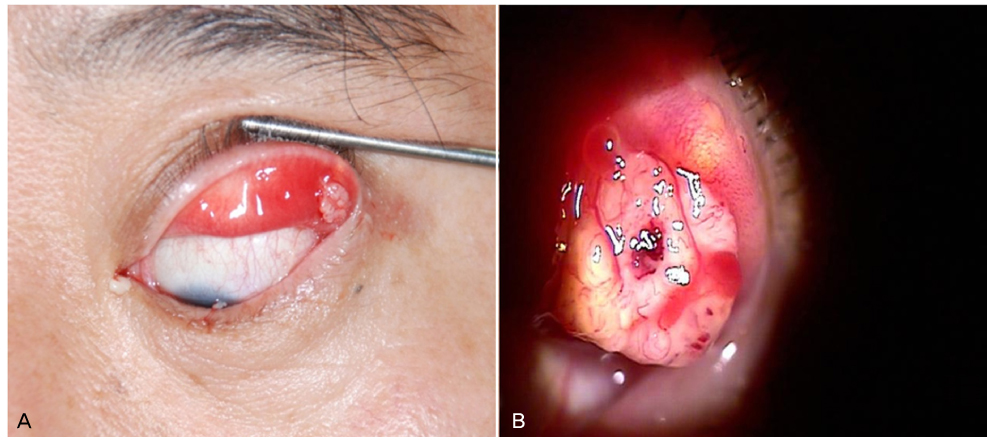
Fig. 2 A yellowish, soft, multi-lobulated mass is shown. The mass protrudes through the lateral end of the left upper palpebral conjunctiva. (A) Gross view. (B) Slit-lamp view.
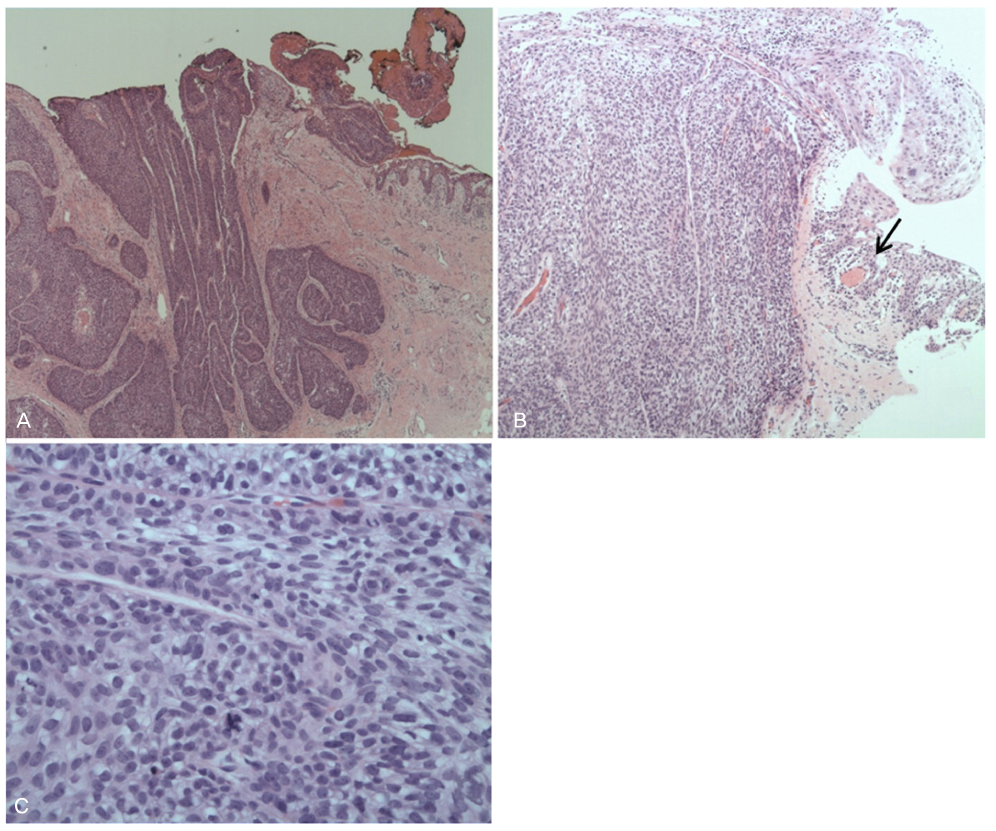
Fig. 3 Histology of the mass. (A) The section revealed a trabecular growth pattern of tumor cell nests (H&E, ×40). (B, C) The cells were characterized by clear cytoplasm, prominent nucleoli, frequent mitoses, few atypical tripolar mitoses, and focal necrosis. There were also foci of trichilemmal keratinization (black arrow) (B: H&E, ×100; C: H&E, ×400).
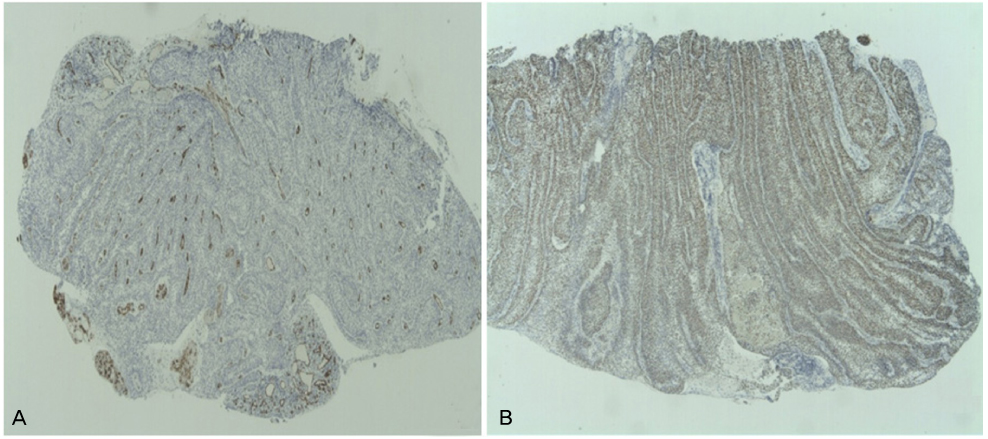
Fig. 4 Immunohistochemical staining of the mass. (A) Negative staining for CD 34. (B) Strongly positive staining for p53.
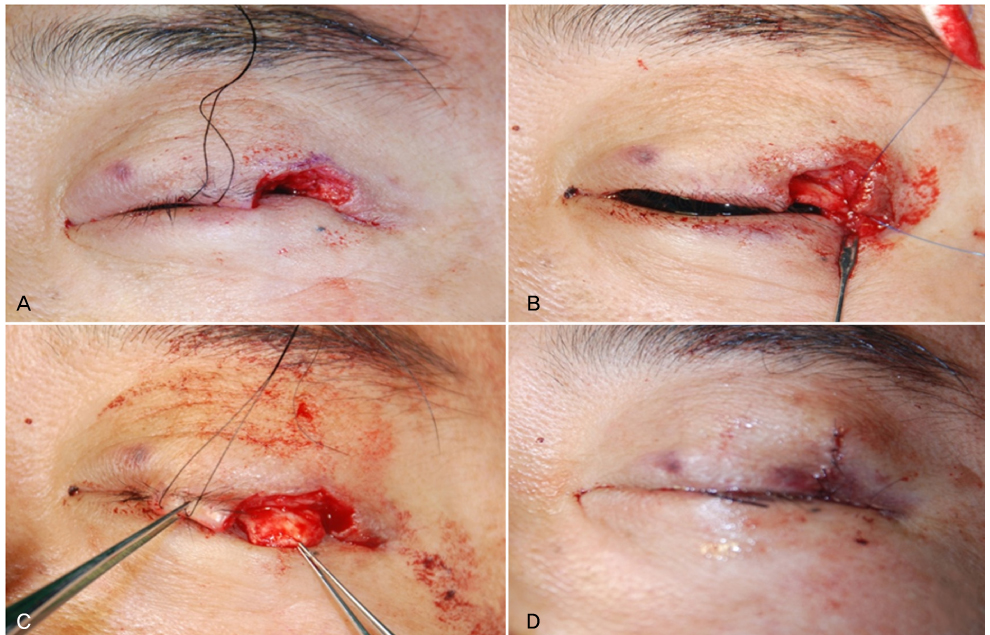
Fig. 5 Mass excision and reconstruction of the defect. (A) Complete mass excision using a pentagonal shape. Tumor-free margins were confirmed by frozen section biopsy. (B) Reconstruction of the posterior lamella with a tarsoconjunctival sling. (C) Reconstruction of the anterior lamella with a myocutaneous advancement flap. (D) Complete closure of the defect.
Reference
-
1. Billingsley EM, Davidowski TA, Maloney ME. Trichilemmal carcinoma. J Am Acad Dermatol. 1997. 36:107–109.2. Reis JP, Tellechea O, Cunha MF, Baptista AP. Trichilemmal carcinoma: review of 8 cases. J Cutan Pathol. 1993. 20:44–49.3. Headington JT. Tumour of the hair follicle: a review. Am J Pathol. 1976. 85:479–514.4. Song MG, Min HG, Jung SY, et al. Trichilemmal carcinoma with a cutaneous horn. Br J Dermatol. 2000. 143:646–647.5. Dailey JR, Helm KF, Goldberg SH. Tricholemmal carcinoma of the eyelid. Am J Ophthalmol. 1993. 115:118–119.6. Lee SJ, Choi KH, Han JH, et al. Malignant proliferating trichilemmal tumor of the lower eyelid. Ophthal Plast Reconstr Surg. 2005. 21:349–352.7. Boscaino A, Terrancciano LM, Donofrio V, et al. Trichilemmal carcinoma: a study of seven cases. J Cutan Pathol. 1992. 19:94–96.8. Swanson PE, Marrogi AJ, Williams DJ, et al. Tricholemmal carcinoma: a clinicopathologic study of 10 cases. J Cutan Pathol. 1992. 19:100–109.9. Chan KO, Lim IJ, Baladas HG, et al. Multiple tumour presentation of trichilemmal carcinoma. Br J Plast Surg. 1999. 52:665–667.10. Lai TF, Huilgol SC, James CL, et al. Trichilemmal carcinoma of the upper eyelid. Acta Ophthalmol Scand. 2003. 81:536–538.11. Masayuki T, Hideo N, Yurihisa I, et al. Surgical treatment of recurrent trichilemmal carcinoma of the upper eyelid. Otolaryngol Head Neck Surg (Tokyo). 2004. 76:709–713.12. Takata M, Rehman I, Rees JL. A trichilemmal carcinoma arising from a proliferating trichilemmal cyst: the loss of the wild-type p53 is a critical event in malignant transformation. Human Pathology. 1998. 29:193–195.13. Poblet E, Jimenez-Acosta F, Rocamora A. QBEND/10 (anti-CD34 antibody) in external root sheath cells and follicular tumours. J Cutan Pathol. 1994. 21:224–228.14. Herrero J, Monteagudo C, Ruiz A, Llombart-Bosch A. Malignant proliferating trichilemmal tumours: an histopathological and immunohistochemical study of three cases with DNA ploidy and morphometric evaluation. Histopathology. 1998. 33:542–546.
