MR Imaging of Congenital Heart Diseases in Adolescents and Adults
- Affiliations
-
- 1Department of Radiology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. yhchoe@smc.samsung.co.kr
- KMID: 754096
- DOI: http://doi.org/10.3348/kjr.2001.2.3.121
Abstract
- Echocardiography and catheterization angiography suffer certain limitations in the evaluation of congenital heart diseases in adults, though these are overcome by MRI, in which a wide field-of view, unlimited multiplanar imaging capability and three-dimensional contrast-enhanced MR angiography techniques are used. In adults, recently introduced fast imaging techniques provide cardiac MR images of sufficient quality and with less artifacts. Ventricular volume, ejection fraction, and vascular flow measurements, including pressure gradients and pulmonary-to-systemic flow ratio, can be calculated or obtained using fast cine MRI, phase-contrast MR flow-velocity mapping, and semiautomatic analysis software. MRI is superior to echocardiography in diagnosing partial anomalous pulmonary venous connection, unroofed coronary sinus, anomalies of the pulmonary arteries, aorta and systemic veins, complex heart diseases, and postsurgical sequelae. Biventricular function is reliably evaluated with cine MRI after repair of tetralogy of Fallot, and Senning's and Mustard's operations. MRI has an important and growing role in the morphologic and functional assessment of congenital heart diseases in adolescents and adults.
MeSH Terms
Figure
-
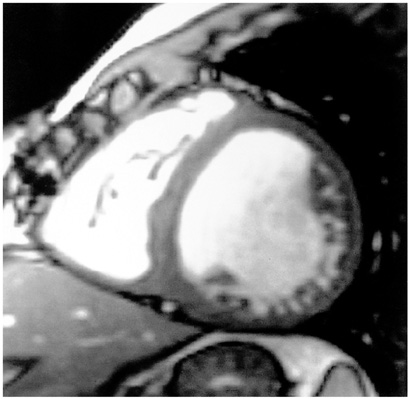
Fig. 1 Diastolic phase short-axial image obtained using the FIESTA technique shows excellent blood-tissue contrast.
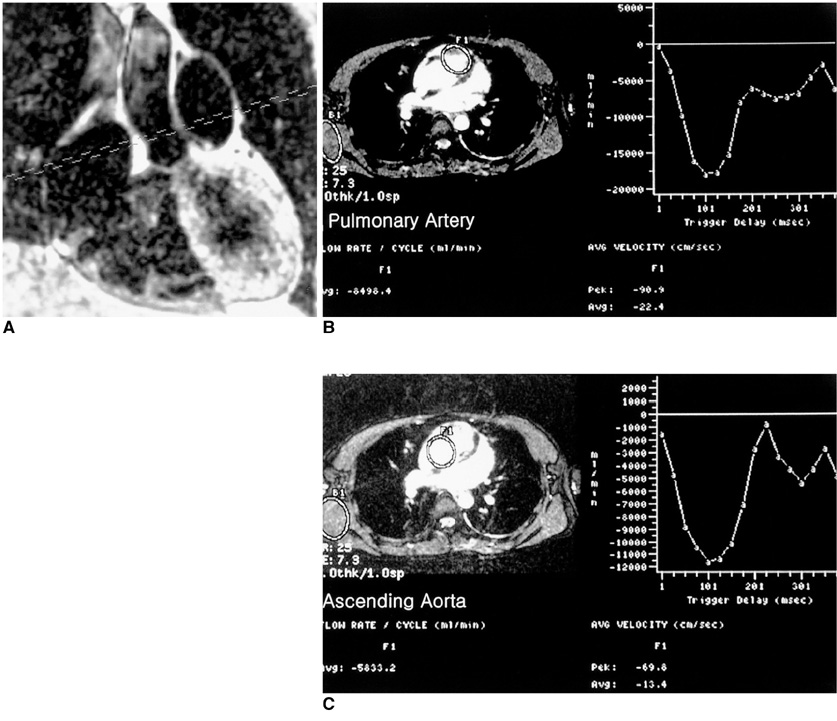
Fig. 2 Calculation of pulmonary-to-systemic arterial flow ratio (Qp/Qs) using velocity-encoded phase-contrast cine MRI in a 24-year-old female with a secundum atrial septal defect. A. An imaging plane perpendicular to the long axes of the aorta and main pulmonary artery is prescribed. B, C. ROIs were drawn on the pulmonary artery and aorta on the cine images (magnitude images on the left plots of B, C). Curves on the right plots show flow volume versus ECG-trigger delay time. Flow volume of the pulmonary artery and aorta was 8,498 ml/min and 5,833 ml/min, respectively, with a Qp/Qs of 1.5. In this patient, the Qp/Qs determined by radioisotope study was 1.7.
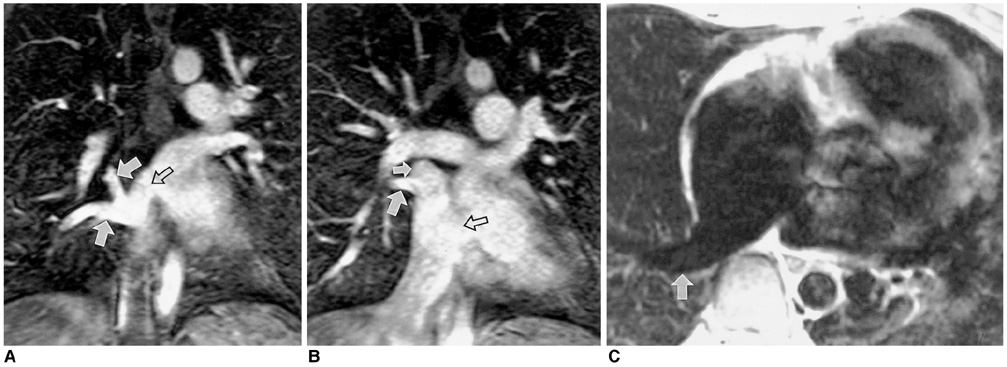
Fig. 3 41-year-old female with partial anomalous pulmonary venous connection of right pulmonary veins to the right atrium and two atrial septal defects. A, B. Coronal source images obtained by contrast-enhanced MR angiography clearly show right upper and middle pulmonary veins (solid arrows) connected with the right atrium. Two atrial septal defects (open arrows) are also visible. C. Axial double inversion-recovery images show the right lower pulmonary vein (arrow) connected with the right atrium.
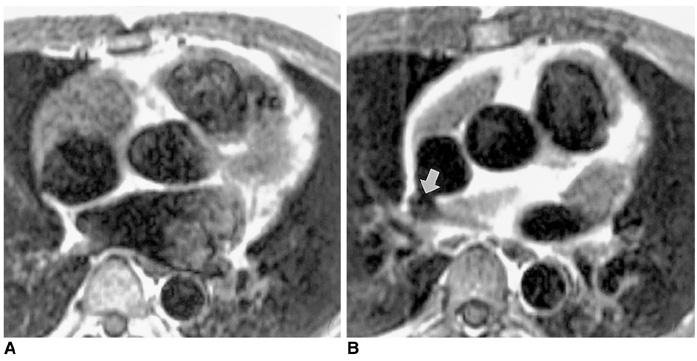
Fig. 4 Small, tricky, atrial septal defect in a 44-year-old male. Transthoracic and transesophageal echocardiography failed to depict the atrial septal defect in spite of clinical suspicion of a left-to-right shunt. A. Axial spin-echo MR image shows intact interatrial septum at the level of the aortic valve. B. Spin-echo image cephalad to A shows a small defect (arrow) in the periphery of the interatrial septum near the junction with the superior vena cava.
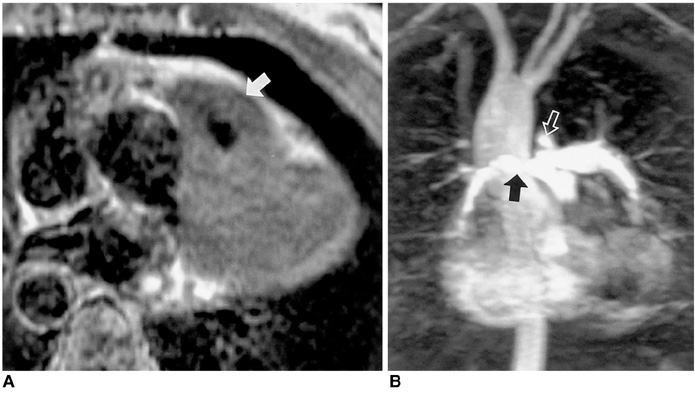
Fig. 5 Tetralogy of Fallot in a 37-year-old female. MRI rather than catheter angiography was performed prior to surgery. A. Axial spin-echo MR image shows severe infundibular stenosis (arrow). B. Three-dimensional contrast-enhanced MR angiography shows small right pulmonary artery (solid arrow) and a ductus diverticulum (open arrow). Note, too, the right-sided aortic arch with mirror image branching.
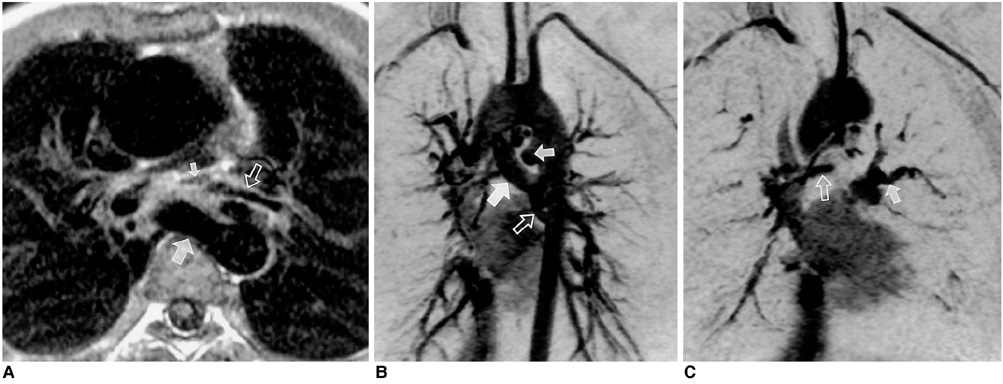
Fig. 6 Pulmonary atresia with ventricular septal defect in a 14-year-old female. MRI was performed to evaluate the size and number of aortopulmonary collateral arteries and to verify the presence of central pulmonary arteries (A, spin-echo image; B and C, three-dimensional images obtained by contrast-enhanced MR angiography with partial volume reconstruction). A major collateral aortopulmonary artery (large solid arrow in A, B) arises from the descending thoracic aorta. Note, too, the presence of another collateral artery (small solid arrow in B) just distal to the aortic arch and small collateral arteries (open arrows in A, B and solid arrow in C). Small central pulmonary arteries (small arrow in A, open arrow in C) with stenosis in the confluent segment are demonstrated by spin-echo imaging and three-dimensional MR angiography.
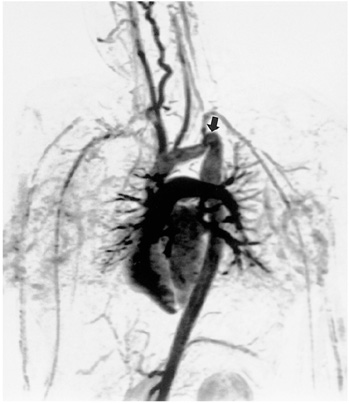
Fig. 7 Tubular hypoplasia of the aortic arch and coarctation in a 17-year-old female. Maximal intensity projection image obtained by contrast-enhanced MR angiography clearly shows arch hypoplasia and coarctation (arrow). This patient also suffered intracerebral hemorrhage, probably associated with coarctation.
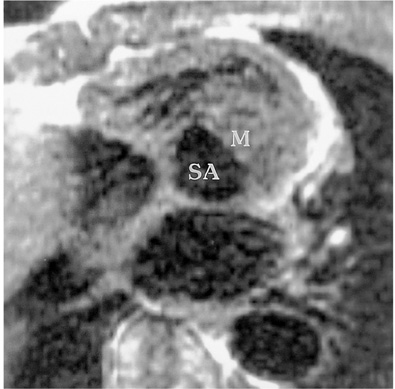
Fig. 8 Subaortic stenosis associated with coarctation of the aorta in a 14-year-old male. Short-axis spin-echo MR image demonstrates subaortic stenosis (SA) due to hypertrophied anterolateral muscle (M).
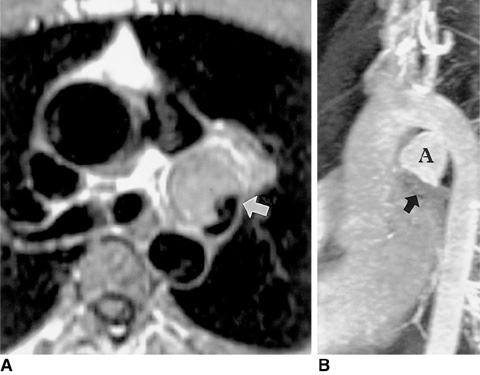
Fig. 9 Aneurysm of the ductus arteriosus in a 31-year-old male. A. Axial spin-echo MR image shows a large aneurysm (arrow) with slow flow within. Spin-echo images do not clearly indicate the origin of this aneurysm. B. Three-dimensional contrast-enhanced MR angiography depicts a bell-shaped aneurysm (A) connected with the aorta. Poor opacification of the hypoplastic left pulmonary artery (arrow) suggests closure of the pulmonary arterial end of the ductus arteriosus.
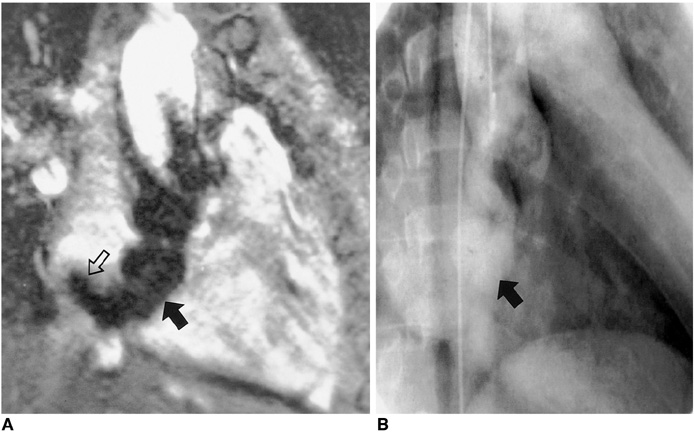
Fig. 10 Rupture of an aneurysm of the sinus of Valsalva in a 42-year-old male. A. Cine MR image in the oblique coronal plane. Turbulent flow (open arrow) is demonstrated as signal voids in the right atrium emanating from the tip of the 'windsock' (solid arrow). B. Conventional cine angiography performed after MRI also shows the ruptured aneurysm of the coronary sinus. Due to low image contrast between the cardiac chambers and aneurysm, the 'windsock' is barely perceptible, however. Surgical findings confirmed the presence of a 4-cm long aneurysm of the sinus of Valsalva and a 0.5-cm-sized tear at the tip of the aneurysm.

Fig. 11 Ebstein's anomaly of the tricuspid valve in a 17-year-old female. A. Oblique axial spin-echo image shows displaced attachment (thick arrow) of the posterior leaflet (thin arrows). B. Conventional cine MR image in the oblique coronal plane shows a large signal void area due to severe tricuspid regurgitation.

Fig. 12 Unroofed coronary sinus in a 24-year-old male. A. Axial spin-echo MR image shows an enlarged coronary sinus (arrow). B. Oblique sagittal planes were selected for imaging of the coronary sinus and left atrium. C. Coronary sinus view, as prescribed in B, shows a large defect (arrow) in the wall between the coronary sinus (CS) and left atrium (LA).
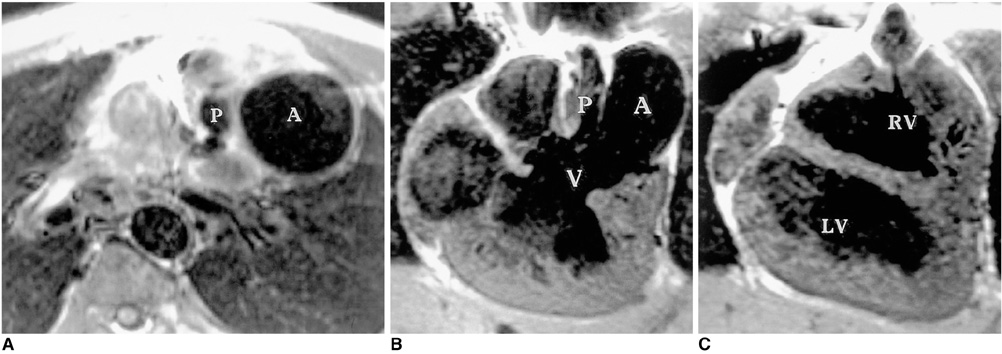
Fig. 13 Corrected transposition in a 14-year-old male. A. Axial spin-echo image shows the left-sided aorta (A) alongside the hypoplastic pulmonary artery (P). B, C. Coronal spin-echo images show a large ventricular septal defect (V) and aorta (A) arising from the left-sided and superiorly located hypoplastic right ventricle (RV). LV, left ventricle
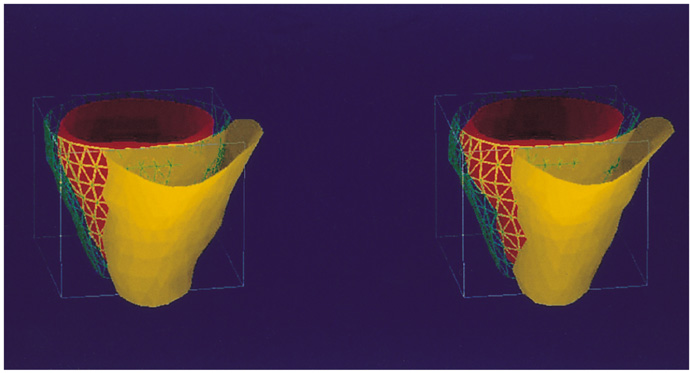
Fig. 14 Biventricular function evaluation using fast cine MR imaging and semi-automated ventricular function analysis software. This 22-year-old male has undergone surgical repair for tetralogy of Fallot and now presents with decreased biventricular function and pulmonary regurgitation. The figure shows three-dimensional images of the right (yellow) and left (red) ventricles in diastolic (left image) and systolic (right image) phases. The three-dimensional volume ejection fraction calculated by this technique was 20.1% and 20.0% for right and left ventricles, respectively.
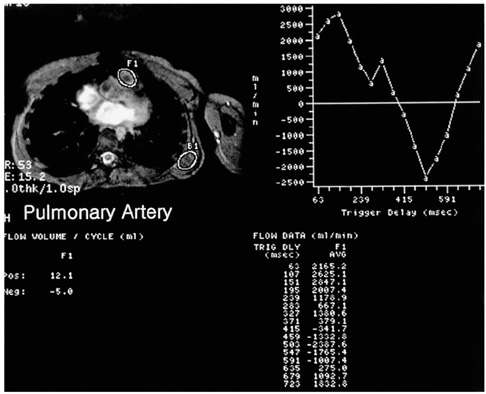
Fig. 15 Estimation of the severity of pulmonary regurgitation after repair of tetralogy of Fallot using velocity-encoded cine MRI. The curve on the right plots pulmonary arterial flow against ECG-trigger delay time. The area between the baseline and the curve below the baseline represents regurgitant volume.
Reference
-
1. Higgins CB, Byrd BF, McNamara M, et al. Magnetic resonance imaging of the heart: a review of the experience in 172 subjects. Radiology. 1985. 155:671–679.2. Didier D, Higgins CB, Fisher MR, Osaki L, Silverman NH, Cheitlin MD. Congenital heart disease: gated MR imaging in 72 patients. Radiology. 1986. 158:227–235.3. Diethelm L, Dery R, Lipton MJ, Higgins CB. Atrial-level shunts: sensitivity and specificity of MR in diagnosis. Radiology. 1987. 162:181–186.4. Gomes A, Lois JF, Williams RG. Pulmonary arteries: MR imaging in patients with congenital obstruction of the right ventricular outflow tract. Radiology. 1990. 174:51–57.5. Jacobstein MD, Fletcher BD, Nelson AD, Clampitt M, Alfidi RJ, Riemenschneider TA. Magnetic resonance imaging: evaluation of palliative systemic-pulmonary artery shunt. Circulation. 1984. 70:650–656.6. Fletcher BD, Jacobstein MD. MRI of congenital abnormalities of the great vessels. AJR. 1986. 146:941–948.7. Julsrud PR, Ehman RL, Hagler DJ, Ilstrup DM. Extracardiac vasculature in candidates for Fontan surgery: MR imaging. Radiology. 1989. 173:503–506.8. Masui T, Seelos KC, Kersting-Sommerhoff BA, Higgins CB. Abnormalities of the pulmonary veins: evaluation with MR imaging and comparison with cardiac angiography and echocardiography. Radiology. 1991. 181:645–649.9. Yoo S-J, Lim TH, Park I-S, et al. MR anatomy of ventricular septal defect in double-outlet right ventricle with situs solitus and atrioventricular concordance. Radiology. 1991. 181:501–505.10. Yoo S-J, Seo J-W, Lim TH, et al. Hearts with twisted atrioventricular connections: findings at MR imaging. Radiology. 1993. 188:109–113.11. Kersting-Sommerhoff BA, Seelos KC, Hardy C, Kondo C, Higgins SS, Higgins CB. Evaluation of surgical procedures for cyanotic congenital heart disease by using MR imaging. AJR. 1990. 155:259–266.12. Vick GW III, Rockey R, Huhta JC, Mulvagh SL, Johnston DL. Nuclear magnetic resonance imaging of the pulmonary arteries, subpulmonic region, and aorticopulmonary shunts: a comparative study with echocardiography and angiography. Am Heart J. 1990. 119:1103–1110.13. Lynch DA, Higgins CB. MR imaging of unilateral pulmonary artery anomalies. J Comput Assist Tomogr. 1990. 14:187–191.14. Vesely TM, Julsrud PR, Brown JJ, Hagler DJ. MR imaging of partial anomalous pulmonary venous connections. J Comput Assist Tomogr. 1991. 15:752–756.15. Choe YH, Lee HJ, Kim HS, Ko JK, Kim JE, Han JJ. MRI of total anomalous pulmonary venous connections. J Comput Assist Tomogr. 1994. 18:243–249.16. Kim TK, Choe YH, Kim HS, et al. Anomalous origin of the right pulmonary artery from the ascending aorta: diagnosis by magnetic resonance imaging. Cardiovasc Intervent Radiol. 1985. 18:118–121.17. Kersting-Sommerhoff BA, Diethelm L, Teitel DF, et al. Magnetic resonance imaging of congenital heart disease: sensitivity and specificity using receiver operating characteristic curve analysis. Am Heart J. 1989. 118:155–161.18. Choe YH, Kim YM, Han BK, Park KG, Lee HJ. MR imaging in the morphologic diagnosis of congenital heart disease. RadioGraphics. 1997. 17:403–422.19. Niezen RA, Helbing WA, Van der Wall EE, Van der Geest RJ, Rebergen SA, De Roos A. Biventricular systolic function and mass studied with MR imaging in children with pulmonary regurgitation after repair for tetralogy of Fallot. Radiology. 1996. 201:135–140.20. Task force of the European Society of Cardiology, in collaboration with the Association of European Paediatric Cardiologists. The clinical role of magnetic resonance imaging in cardiovascular disease. Eur Heart J. 1998. 19:19–31.21. Choi YH, Park JH, Choe YH, Yoo SJ. MR imaging of Ebstein's anomaly of the tricuspid valve. AJR. 1994. 163:539–543.22. Choe YH, Ko JK, Lee HJ, Kang I-S, Park PW, Lee YT. MR imaging of non-visualized pulmonary arteries at angiography in patients with congenital heart disease. J Korean Med Sci. 1998. 13:597–602.23. Ferrari VA, Scott CH, Holland GA, Axel L, Sutton M. Ultrafast three-dimensional contrast-enhanced magnetic resonance angiography and imaging in the diagnosis of partial anomalous pulmonary venous drainage. J Am Coll Cardiol. 2001. 37:1120–1128.24. Taylor AM, Thorne SA, Rubens MB, et al. Coronary artery imaging in grown-up congenital heart disease. Complementary role of magnetic resonance and X-ray coronary angiography. Circulation. 2000. 101:1670–1678.25. Wexler L, Higgins CB. The use of magnetic resonance imaging in adults with congenital heart disease. Am J Card Imaging. 1995. 9:15–28.26. Hartnell GG, Notarianni M. MRI and echocardiography: how do they compare in adults? Sem Roentgenol. 1998. 33:252–261.27. Hartnell GG, Cohen MC, Meier RA, Finn JP. Magnetic resonance angiography demonstration of congenital heart disease in adults. Clin Radiol. 1996. 51:851–857.28. Hoppe UC, Dederichs B, Deutsch HJ, Theissen P, Schicha H, Sechtem U. Congenital heart disease in adults and adolescents: comparative value of transthoracic and transesophageal echocardiography and MR imaging. Radiology. 1996. 199:669–677.29. Pettigrew RI, Oshinski JN, Chatzimavroudis G, Dixon WT. MRI techniques for cardiovascular imaging. J Magn Reson Imaging. 1999. 10:590–601.30. Reeder SB, Du YP, Lima JAC, Bluemke DA. Advance cardiac MR imaging of ischemic heart disease. RadioGraphics. 2001. 21:1047–1074.31. Lee JJ, Tirman PJ, Chang Y, et al. The optimization of scan timing for contrast-enhanced magnetic resonance angiography. Korean J Radiol. 2000. 1:142–151.32. Lee JJ, Chang Y, Kang D-S. Contrast-enhanced magnetic resonance angiography: does the test dose bolus represent the main dose bolus accurately? Korean J Radiol. 2000. 1:91–97.33. Greene R, Miller SW. Cross-sectional imaging of silent pulmonary venous anomalies. Radiology. 1986. 159:279–281.34. White CS, Baffa JM, Haney PJ, Campbell AB, NessAvier M. Anomalies of pulmonary veins: usefulness of spin-echo and gradient-echo MR images. AJR. 1998. 170:1365–1368.35. Hartnell GG, Meier RA. MR angiography of congenital heart disease in adults. RadioGraphics. 1995. 15:781–794.36. Mirowitz SA, Lee JKT, Gutierrez FR, et al. 'Pseudocoarctation' of the aorta: pitfall on cine MR imaging. J Comput Assist Tomogr. 1990. 14:753–755.37. Coard KCM, Martin MP. Ruptured saccular pulmonary artery aneurysm associated with persistent ductus arteriosus. Arch Path Lab Med. 1992. 116:159–161.38. Rominger MB, Bachmann GF, Pabst W, Rau WS. Right ventricular volumes and ejection fraction with fast cine MR imaging in breath-hold technique: applicability, normal values from 52 volunteers, and evaluation of 325 adult cardiac patients. J Magn Reson Imaging. 1999. 10:908–918.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- MR Imaging of Congenital Heart Disease
- Special Report: A 21-Year Publication Analysis of Congenital Heart CT and MRI Articles
- Differential Diagnosis of Congenital Heart Diseases
- Rehabilitation of Children with Congenital Heart Disease: From Children to Adolescents and Adults
- Computer-Assited Instruction : MR Imaging of Congenital Heart Disease
