The Role of Sonography in Patients with Breast Cancer Presenting as an Axillary Mass
- Affiliations
-
- 1Department of Diagnostic Radiology, Yonsei University College of Medicine, Seoul, Korea. ekkim@yumc.yonsei.ac.kr
- 2Department of General Surgery, Yonsei University College of Medicine, Seoul, Korea. ekkim@yumc.yonsei.ac.kr
- KMID: 754061
- DOI: http://doi.org/10.3348/kjr.2002.3.3.189
Abstract
OBJECTIVE
To compare sonography and mammography in terms of their diagnostic value in breast cancer cases which initially presented as an axillary mass without a palpable mass or other clinical symptoms.
MATERIALS AND METHODS
Seven patients with enlarged axillary lymph nodes who first presented with no evidence of palpable breast lesions and who underwent both mammography and sonography were enrolled in this study. In six of the seven, the presence of metastatic adenocarcinoma was confirmed preoperatively by axillary needle aspiration biopsy; in four, subsequent sonographicallyguided breast core biopsy performed after careful examination of the primary site indicated that primary breast cancer was present. In each case, the radiologic findings were evaluated by both breast sonography and mammography.
RESULTS
Breast lesions were detected mammographically in four of seven cases (57%); in three of the four, the lesion presented as a mass, and in one as microcalcification. In three of these four detected cases, fatty or scattered fibroglandular breast parenchyma was present; in one, the parenchyma was dense. In the three cases in which lesions were not detected, mammography revealed the presence of heterogeneously dense parenchyma. Breast sonography showed that lesions were present in six of seven cases (86%); in the remaining patient, malignant microcalcification was detected at mammography. Final pathologic examination indicated that all breast lesions except one, which was a ductal carcinoma in situ, with microinvasion, were infiltrating ductal carcinomas whose size ranged from microscopic to greater than 3 cm. At the time of this study, all seven patients were alive and well, having been disease free for up to 61 months after surgery.
CONCLUSION
In women with a palpable axillary mass confirmed as metastatic adenocarcinoma, breast sonography may be a valuable adjunct to mammography.
MeSH Terms
-
Adenocarcinoma/radiography/secondary/*ultrasonography
Adult
Axilla/*pathology
Biopsy, Needle
Breast/*pathology
Breast Neoplasms/pathology/radiography/*ultrasonography
Carcinoma, Infiltrating Duct/pathology/radiography/*ultrasonography
Carcinoma, Intraductal, Noninfiltrating/pathology/radiography/*ultrasonography
Female
Human
Lymph Nodes/radiography/*ultrasonography
Mammography
Middle Age
Ultrasonography, Mammary
Figure
-

Fig. 1 A 64-year-old woman with axillary node metastasis. A. Mammography reveals not only enlarged nodes but also scattered fibroglandular parenchyma, with a 1-cm spiculated nodule in the right upper outer quadrant (arrow). B. At sonography, multiple enlarged axillary lymph nodes are seen, the largest of which has a diameter of approximately 3.5 cm. C. At the corresponding site of mammographic abnormality, sonography depicts a 1cm-sized hypoechoic nodule, confirmed to be an infiltrating ductal carcinoma.
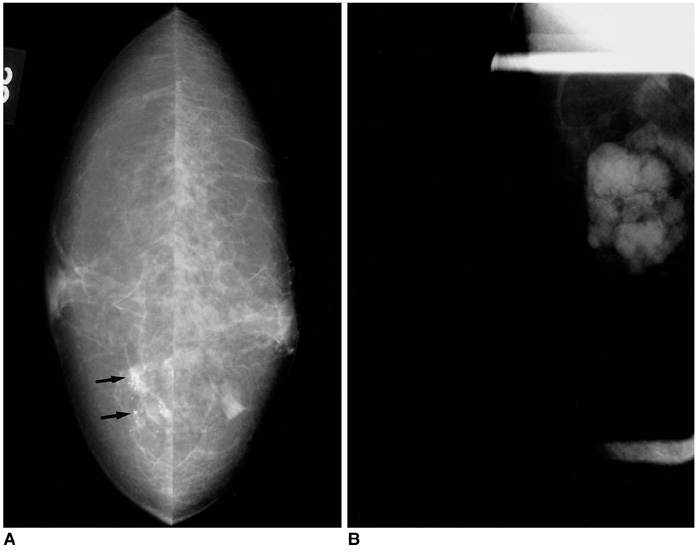
Fig. 2 A 48-year-old-woman with axillary node metastasis. A. Mammography reveals the presence of clustered microcalcifications (arrows), without mass, in the right inner central area. At sonography, however, neither a breast nodule nor the above-mentioned microcalcifications are seen. Surgical excision after needle localization confirmed the presence of ductal carcinoma in situ, with microinvasion. B. Axillary view depicts multiple hyperdense enlarged lymph nodes.
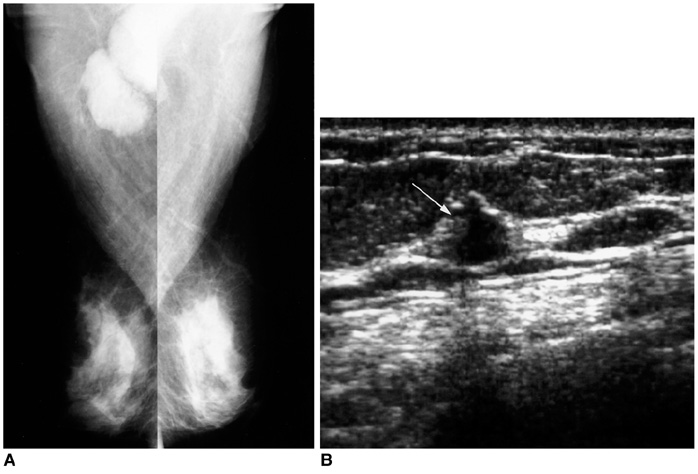
Fig. 3 A 60-year-old woman with axillary node metastasis. A. Mammography demonstrates heterogeneous fibroglandular densities, with no sign of malignancy. The right axillary lymph nodes are, however, enlarged. B. Careful examination of this sonogram shows that the right upper central area contains a malignant microlobulated nodule, 1cm in diameter (arrow). Sonograpahically-guided core biopsy confirmed the presence of an infiltrating ductal carcinoma.
Reference
-
1. Halsted WS. The results of radical operations for the cure of carcinoma of the breast. Ann Surg. 1907. 46:1–19.2. Fourquet A, De La Rochefordiere A, Campana F. Harris JR, Lippman ME, Morrow M, Hellman S, editors. Occult primary cancer with axillary metastases. Diseases of the breast. 1996. Philadelphia: Lippincott-Raven;892–896.3. Solin LJ. Fowble B, Goodman RL, Glick JH, Rosato EF, editors. Special considerations. Breast cancer treatment: a comprehensive guide to mangement. 1991. St Louis: Mosby-Year Book;523–528.4. Patel J, Nemoto T, Rosner D, Dao TL, Pickren JW. Axillary lymph node metastasis from an occult breast cancer. Cancer. 1981. 47:2923–2927.5. Orel SG, Schnall MD, Powell CM, et al. Staging of suspected breast cancer: effect of MR imaging and MR-guided biopsy. Radiology. 1995. 196:115–122.6. Orel SG, Weinstein SP, Schnall MD, et al. Breast MR imaging in patients with axillary node metastases and unknown primary malignancy. Radiology. 1999. 212:543–549.7. Fieuerman L, Attie JN, Rosenberg B. Carcinoma in axillary lymph nodes as an indicator of breast cancer. Surg Gynecol Obstet. 1962. 114:5–8.8. Baron PL, Moore MP, Kinne DW, Candela FC, Osborne MP, Petrek JA. Occult breast cancer presenting with axillary metastases. Arch Surg. 1990. 125:210–215.9. Orel SG, Hochman MG, Schnall MD, Reynolds C, Sullivan DC. High-resolution MR imaging of the breast: clinical context. RadioGraphics. 1996. 16:1385–1401.10. Obdeijn IM, Brouwers-Kuyper EM, Tilanus-Linthorst MM, Wiggers T, Oudkerk M. MR imaging-guided sonography followed by fine-needle aspiration cytology in occult carcinoma of the breast. AJR. 2000. 174:1079–1084.11. Morris EA, Schwartz LH, Dershaw DD, Van Zee KJ, Abramson AF, Liberman L. MR imaging of the breast in patients with occult primary breast carcinoma. Radiology. 1997. 205:437–440.12. Kolb TM, Lichy J, Newhouse JH. Occult cancer in women with dense breasts: detection with screening US-Diagnostic yield and tumor characteristics. Radiology. 1998. 207:191–199.13. Buchberger W, DeKoekkoek-Doll P, Springer P, Obrist P, Dunser M. Incidental findings on sonography of the breast: clinical significance and diagnostic workup. AJR. 1999. 173:921–927.14. Ashikari R, Rosen PP, Urban JA, Senoo T. Breast cancer presenting as an axillary mass. Ann Surg. 1976. 183:415–417.15. Stavros M, Buckley DL, Horsman A. Prediction of axillary lymph node status in invasive breast cancer with dynamic contrast-enhanced MR imaging. Radiology. 1997. 203:317–321.16. Van Lancker M, Goor C, Sacre R, et al. Patterns of axillary lymph node metastasis in breast cancer. Am J Clin Oncol. 1995. 18:267–272.17. Kambouris AA. Axillary node metastasis in relation to the size and location of breast cancers: analysis of 147 patients. Am Surg. 1996. 62:519–524.18. Rosen EL, Sickles E, Keating D. Ability of mammography to reveal nonpalpable breast cancer in women with palpable breast masses. AJR. 1999. 172:309–312.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Supplementary Screening Sonography in Mammographically Dense Breast: Pros and Cons
- Carcinoma of the Axillary Tail of Spence: A Case Report with Imaging Findings
- The Benefit of Sonography in Pregnancy-associated Breast Cancer
- Hypermetabolic Axillary Mass on 18F FDG PET/CT: Breast Cancer Arising from Accessory Breast Tissue
- Axillary sparganosis which was misunderstood lymph node metastasis during neoadjuvant chemotheraphy in a breast cancer patient
