J Rhinol.
2024 Mar;31(1):22-28. 10.18787/jr.2024.00001.
Do Anatomical Variations Affect the Location of Solitary Sphenoid Sinus Fungal Balls? A 10-Year Retrospective Study
- Affiliations
-
- 1Department of Otorhinolaryngology-Head and Neck Surgery, Nowon Eulji Medical Center, Eulji University School of Medicine, Seoul, Republic of Korea
- 2Department of Otorhinolaryngology-Head and Neck Surgery, Kyung Hee University Hospital, Kyung Hee University College of Medicine, Seoul, Republic of Korea
- KMID: 2554087
- DOI: http://doi.org/10.18787/jr.2024.00001
Abstract
- Background and Objectives
Sinonasal fungal balls (FBs) most commonly occur in the maxillary sinus, followed by the sphenoid sinus (SS). Relatively little is known about the predisposing factors and pathogenesis of unilateral sphenoid sinus fungal balls (SSFBs) compared to maxillary sinus FBs. We investigated whether anatomical variations have clinical implications for the location of unilateral SSFBs.
Methods
This study included 33 patients who underwent endoscopic sinus surgery for unilateral SSFBs between 2010 and 2021. Preoperative computed tomography scans were used to analyze the presence of anatomical variations, including sphenoid lateral recess, complete accessory septum of the SS, types of SS pneumatization, anterior and posterior nasal septal deviation (NSD), cephalocaudal NSD, concha bullosa (CB), Haller cell (HC), paradoxical middle turbinate (MT), everted uncinated process (UP), and Onodi cell.
Results
The presence of HC (33.3% vs. 12.1%, p=0.04), complete accessory septum of the SS (51.6% vs. 25.8%, p=0.04), and the sellar type of the SS (90.9% vs. 50%, p=0.003) differed significantly according to the presence or absence of FBs in the SS. However, other anatomical variations, including NSD, CB, paradoxical MT, everted UP, Onodi cell, and sphenoid lateral recess, were not significantly associated with the presence of unilateral SSFBs (all p>0.05). In the multivariable analysis, only sellar-type pneumatization of the SS showed a statistically significant relationship with SSFB, not the combined conchal and presellar type (adjusted odds ratio, 8.96; 95% confidence interval, 1.27–63.19; p=0.03).
Conclusion
We demonstrated that unilateral SSFBs were most strongly associated with the ipsilateral type of SS pneumatization, followed by the presence of HC and a complete accessory septum of the SS. Intranasal anatomical variations may play a significant role in the location of unilateral SSFBs.
Figure
-

Fig. 1. Anteroposterior (A and B) and cephalocaudal (C) nasal septal deviations. A: Anterior deviation of the nasal septum toward the left at the level of the nasal valve. B: Posterior deviation of the nasal septum toward the left at the level of the ostiomeatal unit. C: Cephalocaudal deviation of the nasal septum toward the right at the level of the both sphenoid ostia. point c, crista galli; point n, anterior nasal spine; point M, midpoint of nasal tip; point R, sphenoidal rostrum.
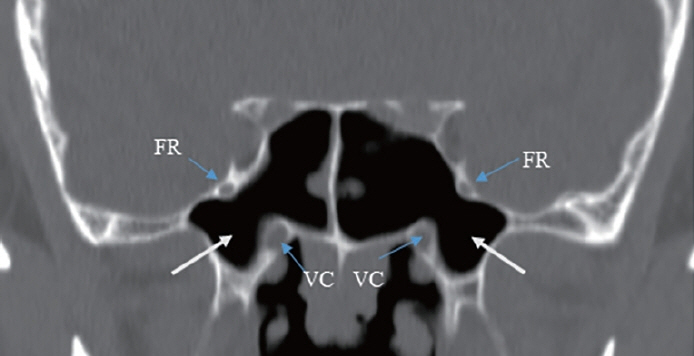
Fig. 2. Sphenoid lateral recess (white arrows). FR, foramen rotundum; VC, vidian canal.
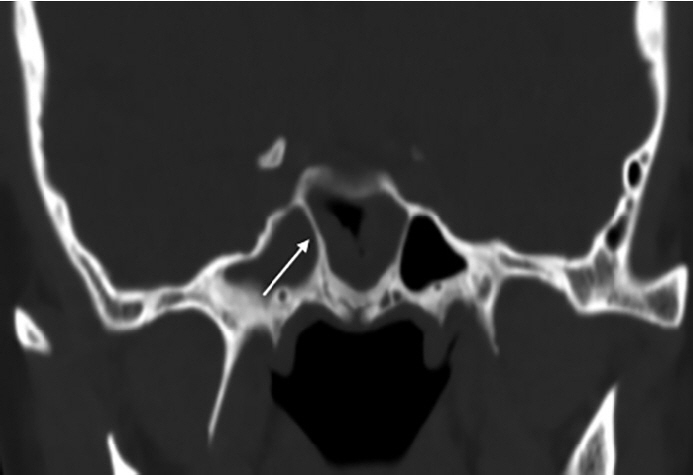
Fig. 3. Right complete accessory sphenoidal septum (white arrow).
Reference
-
References
1. Callejas CA, Douglas RG. Fungal rhinosinusitis: what every allergist should know. Clin Exp Allergy. 2013; 43(8):835–49.
Article2. Montone KT, Livolsi VA, Feldman MD, Palmer J, Chiu AG, Lanza DC, et al. Fungal rhinosinusitis: a retrospective microbiologic and pathologic review of 400 patients at a single university medical center. Int J Otolaryngol. 2012; 2012:684835.
Article3. Nicolai P, Lombardi D, Tomenzoli D, Villaret AB, Piccioni M, Mensi M, et al. Fungus ball of the paranasal sinuses: experience in 160 patients treated with endoscopic surgery. Laryngoscope. 2009; 119(11):2275–9.
Article4. Shin JM, Baek BJ, Byun JY, Jun YJ, Lee JY. Analysis of sinonasal anatomical variations associated with maxillary sinus fungal balls. Auris Nasus Larynx. 2016; 43(5):524–8.
Article5. Costa F, Emanuelli E, Franz L, Tel A, Sembronio S, Robiony M. Fungus ball of the maxillary sinus: retrospective study of 48 patients and review of the literature. Am J Otolaryngol. 2019; 40(5):700–4.
Article6. Tomazic PV, Dostal E, Magyar M, Lang-Loidolt D, Wolf A, Koele W, et al. Potential correlations of dentogenic factors to the development of clinically verified fungus balls: a retrospective computed tomography-based analysis. Laryngoscope. 2016; 126(1):39–43.
Article7. Doo JG, Min HK, Choi GW, Kim SW, Min JY. Analysis of predisposing factors in unilateral maxillary sinus fungal ball: the predictive role of odontogenic and anatomical factors. Rhinology. 2022; 60(5):377–83.
Article8. Hwang SH, Kang JM, Cho JH, Kim BG. What is the relationship between the localization of maxillary fungal balls and intranasal anatomic variations? Clin Exp Otorhinolaryngol. 2012; 5(4):213–7.
Article9. Tsai TL, Guo YC, Ho CY, Lin CZ. The role of ostiomeatal complex obstruction in maxillary fungus ball. Otolaryngol Head Neck Surg. 2006; 134(3):494–8.
Article10. Li L, Han D, Li S, Jr NRL. The association of nasal septal deviation with solitary sphenoidal fungus ball: retrospective analysis of 43 patients. J Otol Rhinol. 2020; 9(7):384.11. Orhan I, Ormeci T, Bilal N, Sagiroglu S, Doganer A. Morphometric analysis of sphenoid sinus in patients with nasal septum deviation. J Craniofac Surg. 2019; 30(5):1605–8.
Article12. Li L, London NR Jr, Prevedello DM, Carrau RL. Endoscopic prelacrimal approach to lateral recess of sphenoid sinus: feasibility study. Int Forum Allergy Rhinol. 2020; 10(1):103–9.
Article13. Aksoy F, Yenigun A, Goktas SS, Ozturan O. Association of accessory sphenoid septa with variations in neighbouring structures. J Laryngol Otol. 2017; 131(1):51–5.
Article14. Gibelli D, Cellina M, Gibelli S, Oliva G, Termine G, Dolci C, et al. Prevalence of accessory septations of sphenoid sinus in pediatric population: applications to endoscopic sinus surgery. Anat Rec (Hoboken). 2020; 303(8):2171–6.
Article15. Alsaied AS. Paranasal sinus anatomy: what the surgeon needs to know. In Gendeh BS, editor. Paranasal Sinuses [Internet]. London: IntechOpen;2017. [cited 2023 Dec 1]. Available from: https://doi.org/10.5772/intechopen.69089.
Article16. Eberhardt JA, Torabinejad M, Christiansen EL. A computed tomographic study of the distances between the maxillary sinus floor and the apices of the maxillary posterior teeth. Oral Surg Oral Med Oral Pathol. 1992; 73(3):345–6.
Article17. Basurrah M, Kim DH, Lee IH, Kim SW, Kim SW. Effects of dental factors on fungal sinusitis. ORL J Otorhinolaryngol Relat Spec. 2022; 84(4):309–14.
Article18. Grosjean P, Weber R. Fungus balls of the paranasal sinuses: a review. Eur Arch Otorhinolaryngol. 2007; 264(5):461–70.
Article19. Lim HS, Yoon YH, Xu J, Kim YM, Rha KS. Isolated sphenoid sinus fungus ball: a retrospective study conducted at a tertiary care referral center in Korea. Eur Arch Otorhinolaryngol. 2017; 274(6):2453–9.
Article20. Alkire BC, Bhattacharyya N. An assessment of sinonasal anatomic variants potentially associated with recurrent acute rhinosinusitis. Laryngoscope. 2010; 120(3):631–4.
Article21. Başer E, Sarioğlu O, İdil M, Çukurova İ, Arslan İB. Effect of sphenoid sinus volume and pneumatization type on isolated chronic sphenoid sinusitis fungi and polyps. Tr-ENT. 2020; 30(2):58–65.
Article22. Illing E, Schlosser RJ, Palmer JN, Curé J, Fox N, Woodworth BA. Spontaneous sphenoid lateral recess cerebrospinal fluid leaks arise from intracranial hypertension, not Sternberg’s canal. Int Forum Allergy Rhinol. 2014; 4(3):246–50.
Article23. Klossek JM, Serrano E, Péloquin L, Percodani J, Fontanel JP, Pessey JJ. Functional endoscopic sinus surgery and 109 mycetomas of paranasal sinuses. Laryngoscope. 1997; 107(1):112–7.
Article24. Kim JS, Kim BK, Hong SD, Kim HJ, Kim HY. Clinical characteristics of sphenoid sinus fungal ball patients with visual disturbance. Clin Exp Otorhinolaryngol. 2016; 9(4):326–31.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Two Cases of Bilateral Paranasal Sinus Fungus Balls with Sphenoid Sinus Involvement
- A Case of Multiple Fungal Balls Involving the Isolated Three Sinuses
- Isolated Sphenoid Fungal Sinusitis With Mucocele Mistaken for Chordoma: A Study of Two Unique Cases
- A Case of Abducens Nerve Palsy Caused by Isolated Sphenoid Fungal Sinusitis
- A Case of Fungal Sphenoid Sinusitis with Visual Loss
