Facilitated Retrograde Access via the Facial Vein for Transvenous Embolization of the Cavernous Sinus Dural Arteriovenous Fistula with Isolated Ophthalmic Venous Drainage
- Affiliations
-
- 1Department of Radiology, College of Medicine, Majmaah University, Al Majmaah, Saudi Arabia
- 2Department of Radiology and Research Institute of Radiology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
- KMID: 2552878
- DOI: http://doi.org/10.5469/neuroint.2023.00493
Abstract
- Management of cavernous sinus dural arteriovenous fistula (CSDAVF) continues to present significant challenges, particularly when the inferior petrosal sinus is thrombosed, collapsed, or angiographically invisible. In this study, we introduce facilitated retrograde access via the facial vein, which is employed in the transvenous embolization of CSDAVF with isolated superior ophthalmic venous drainage. We also present illustrative cases and technical points.
Figure
-
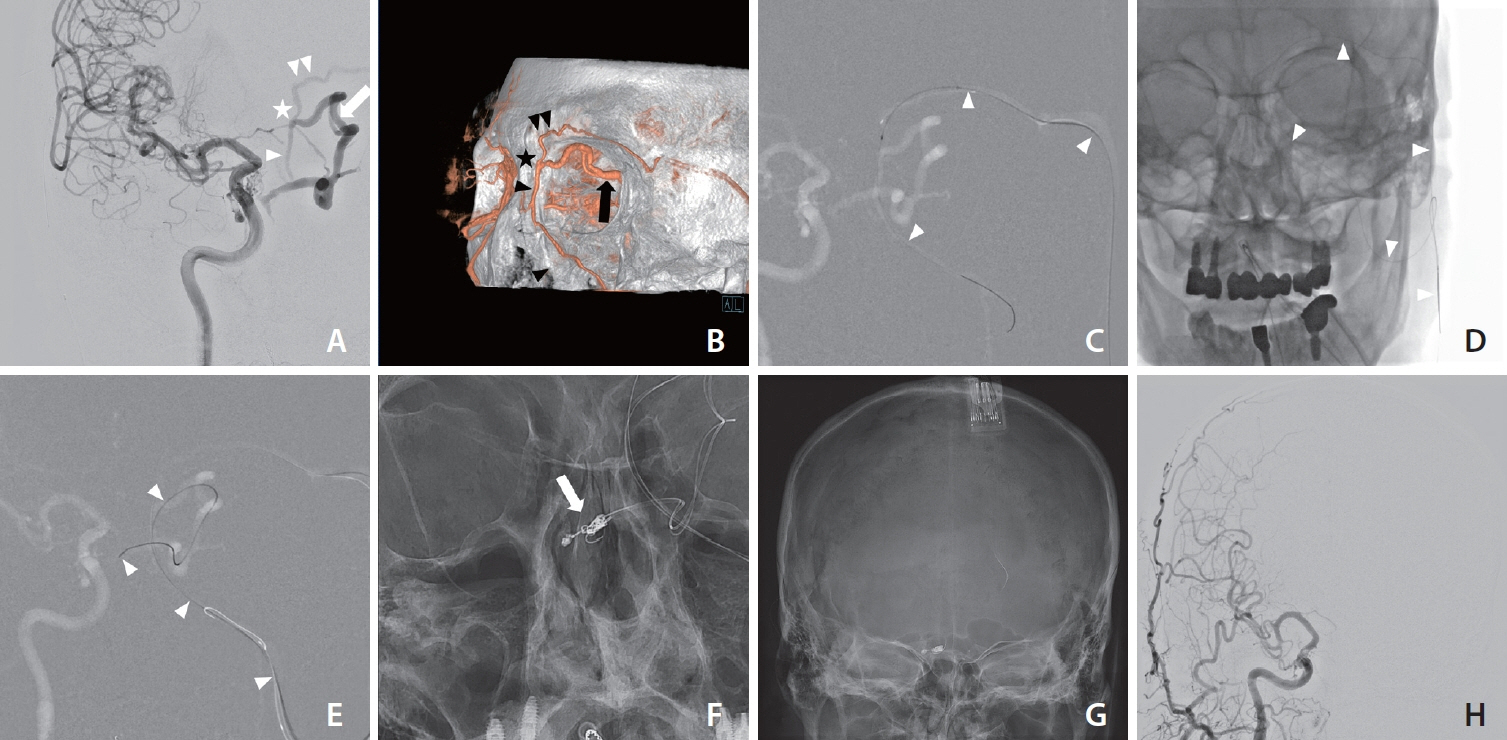
Fig. 1. Case 1: Frontal projection of the right internal carotid arteriogram (A) shows a dural arteriovenous fistula in the right cavernous sinus. The main venous drainage is through an intercavernous sinus to the left superior ophthalmic vein (arrow). The left supraorbital vein (double arrowheads), left angular vein (single arrowhead), and left superior ophthalmic vein (arrow) are connected at the left superomedial orbital rim (asterisk). The volume- rendered image from 3-dimensional rotational angiography (B) shows the acute angle at the junction between the left supraorbital vein (double arrowheads) and the left superior ophthalmic vein (arrow) at the left superomedial orbital rim (asterisk). Single arrowheads denote the left angular vein and the left facial vein. The roadmap image in frontal projection (C) depicts a clear venous drainage path via the left supraorbital vein to the left middle temporal vein, contrary to a less distinct path via the left angular vein to the left facial vein. The microcatheter and microwire (arrowheads) were advanced through the left middle temporal, left supraorbital, and left angular veins. Native image in frontal projection (D) depicts the reentry of the 300-cm microwire (arrowheads) into the retromandibular vein through the transverse facial vein. The roadmap image with the 300-cm microwire in place within the facial and scalp veins (E) guides the second microwire from the left retromandibular vein. Finally, the roadmap in the working projection confirms successful access to the fistula with the second microwire (arrowheads) guided by the 300-cm microwire. Native image in working projection (F) shows Onyx cast and coil mass (arrow) at the fistula. The final right common carotid arteriogram, comprising both native and subtracted images (G, H) in fontal projection, confirms the absence of any residual arteriovenous shunt flow after embolization.

Fig. 2. Case 2: Frontal and lateral projections of the right external carotid arteriogram (A, B) depict a dural arteriovenous fistula in the right cavernous sinus. The only venous drainage route is the engorged right superior ophthalmic artery (arrow). The right supraorbital vein (double arrowheads), right angular vein (single arrowheads), and right superior ophthalmic vein (arrow) are connected at the right superomedial orbital rim (asterisks). Three-dimensional rotational angiography (C, D) of the right external carotid artery depicts an acute angle at the junction between the right supraorbital vein (double arrowheads) and the right superior ophthalmic vein (arrows) at the right superomedial orbital rim (asterisks). Single arrowheads denote the left angular vein. Native images in frontal and lateral projections (E, F) show a guiding catheter (arrows) placed in the right middle temporal vein, one of the tributaries of the right external jugular vein, and a 300-cm microwire (arrowheads) placed in the right middle temporal, right supraorbital, right angular, right common facial, and right internal jugular veins. The final right common carotid arteriogram, comprising both native and subtracted images (G, H) in lateral projection, confirms the absence of any residual arteriovenous shunt flow after coil embolization (arrow).
Reference
-
1. Hou K, Li G, Luan T, Xu K, Yu J. Endovascular treatment of the cavernous sinus dural arteriovenous fistula: current status and considerations. Int J Med Sci. 2020; 17:1121–1130.
Article2. Jia ZY, Song YS, Sheen JJ, Kim JG, Lee DH, Suh DC. Cannulation of occluded inferior petrosal sinuses for the transvenous embolization of cavernous sinus dural arteriovenous fistulas: usefulness of a frontier-wire probing technique. AJNR Am J Neuroradiol. 2018; 39:2301–2306.
Article3. Biondi A, Milea D, Cognard C, Ricciardi GK, Bonneville F, van Effenterre R. Cavernous sinus dural fistulae treated by transvenous approach through the facial vein: report of seven cases and review of the literature. AJNR Am J Neuroradiol. 2003; 24:1240–1246.4. Mounayer C, Piotin M, Spelle L, Moret J. Superior petrosal sinus catheterization for transvenous embolization of a dural carotid cavernous sinus fistula. AJNR Am J Neuroradiol. 2002; 23:1153–1155.5. Quinones D, Duckwiler G, Gobin PY, Goldberg RA, Vinuela F. Embolization of dural cavernous fistulas via superior ophthalmic vein approach. J Neuroophthalmol. 1999; 19:116.
Article6. Dye J, Duckwiler G, Gonzalez N, Kaneko N, Goldberg R, Rootman D, et al. Endovascular approaches to the cavernous sinus in the setting of dural arteriovenous fistula. Brain Sci. 2020; 10:554.
Article7. Bertha A, Suganthy R. Anatomical variations in termination of common facial vein. J Clin Diagn Res. 2011; 5:24–27.8. Cheung N, McNab AA. Venous anatomy of the orbit. Invest Ophthalmol Vis Sci. 2003; 44:988–995.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Transvenous Embolization of Cavernous Sinus Dural Arteriovenous Fistula Using the Direct Superior Ophthalmic Vein Approach: A Case Report
- Middle temporal vein access for transvenous embolization of Cavernous sinus dural arteriovenous fistula: A case report and review of literature
- Transvenous Coil Embolization for Dural Arteriovenous Fistulas of the Ophthalmic Sheath: Report of Two Cases and Review of the Literature
- Transvenous Embolization of Dural Carotid Cavernous Fistula through the Supraorbital Vein
- Reversible Abducens Nerve Palsy Following Transvenous Embolization of Cavernous Sinus Dural Arteriovenous Fistula
