Middle temporal vein access for transvenous embolization of Cavernous sinus dural arteriovenous fistula: A case report and review of literature
- Affiliations
-
- 1Department of Neurosurgery, Keimyung University Dongsan Medical Center, Daegu, Korea
- KMID: 2527594
- DOI: http://doi.org/10.7461/jcen.2021.E2021.06.008
Abstract
- Transvenous endovascular treatment is the first choice for treating most cavernous sinus dural arteriovenous fistulas (CDAVFs). Among several available venous routes, the inferior petrosal sinus is the most commonly used. We report a case of CDAVF treated with endovascular treatment via the middle temporal vein (MTV). A 65-year-old man presented with unilateral chemosis and exophthalmos for approximately two months. Digital subtraction angiography showed a right CDAVF with predominant venous drainage toward the right superior ophthalmic vein. The superior ophthalmic vein primarily drained into the dilated MTV. Both sides of the inferior petrosal sinus were occluded; therefore, transvenous embolization was performed via the MTV route. The fistula was completely obliterated. The patient’s symptoms improved and the postoperative course was uneventful. The transfemoral approach via the MTV to treat CDAVF provides a crucial alternative when other venous routes are difficult or impossible to navigate with a catheter.
Keyword
Figure
-
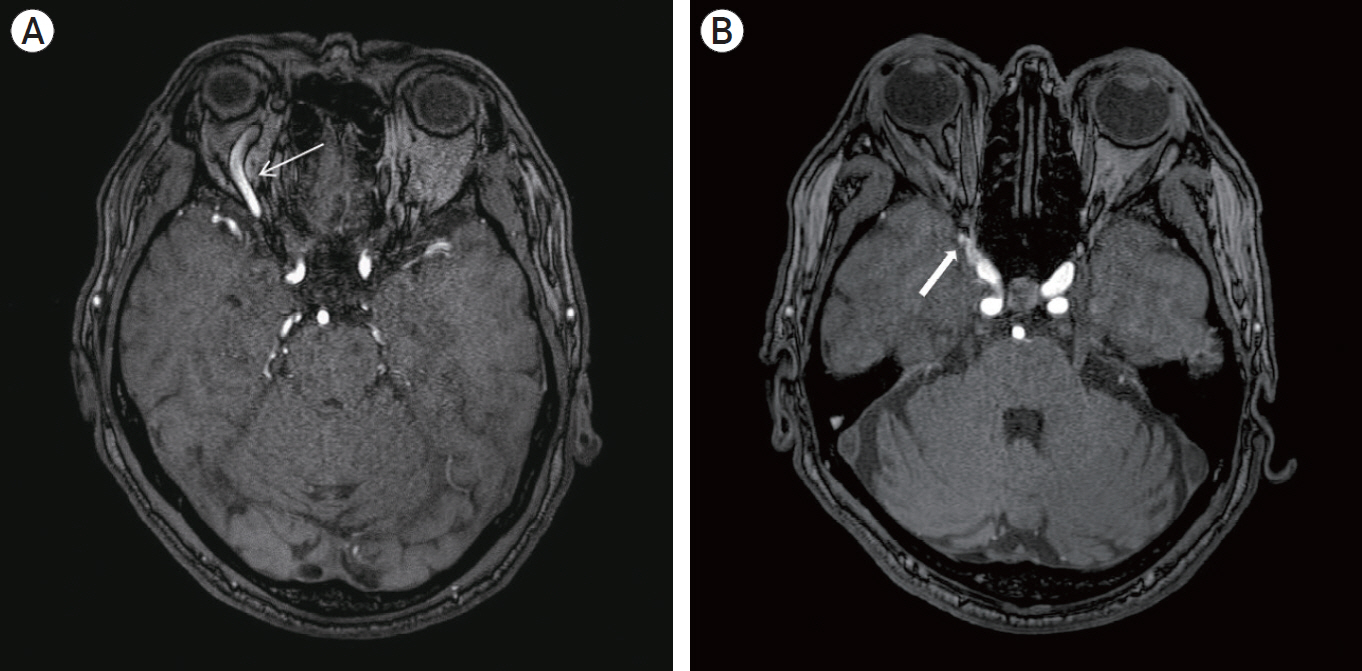
Fig. 1. Axial magnetic resonance angiography source image showing (A) superior ophthalmic vein dilatation (white arrow) with (B) prominent vascularity at the cavernous sinus (thick white arrow).
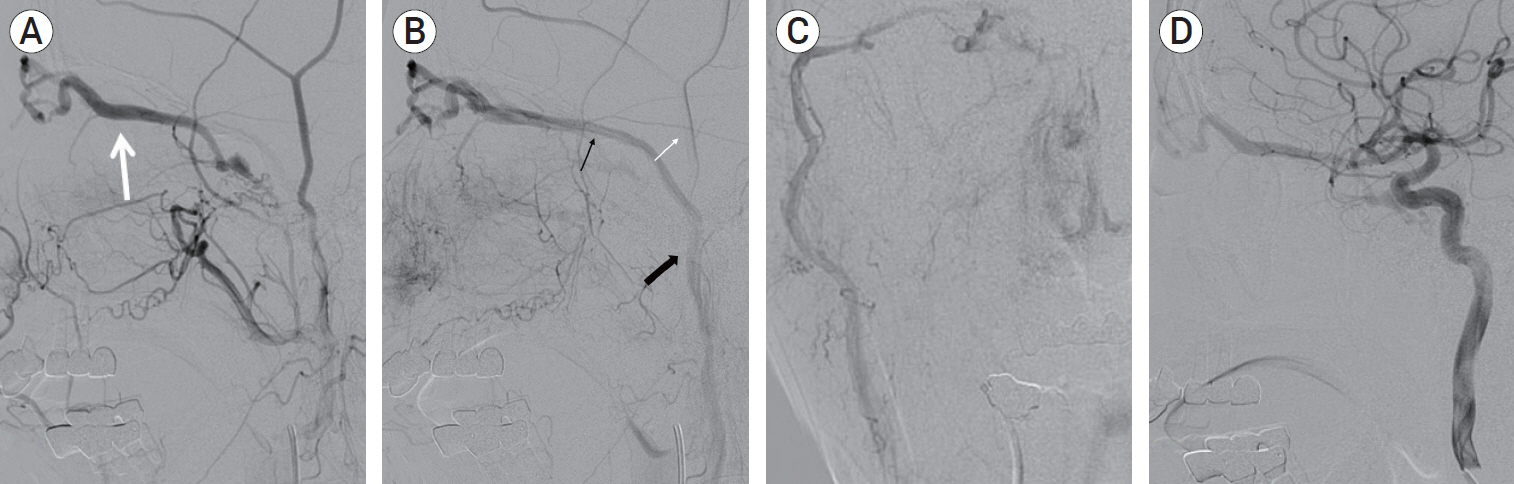
Fig. 2. Right cavernous sinus dural arteriovenous fistula in a 65-year-old man. (A) Lateral-view angiogram from the right external carotid artery, obtained before embolization, shows predominant venous drainage toward the superior ophthalmic vein (white arrow). (B) Lateral-view angiogram from the right external carotid artery shows middle temporal vein dilatation (thin black arrow), superficial temporal vein (white arrow), retromandibular vein (thick black arrow). (C) Anteroposterior-view angiogram of the right external carotid artery. (D) Lateral-view angiogram from the right internal carotid artery shows multiple arterial feeders.

Fig. 3. Lateral-view angiogram of the right external carotid artery showing transvenous embolization via the MTV vein route. (A) A microcatheter advanced into the MTV (thick black arrow) and shows gentle progression to the nasofrontal vein (black arrow). (B) During detachable coil packing at the cavernous sinus. Fistula was completely obliterated with the detachable coil. (C) Angiogram with advanced microcatheter via MTV. MTV, middle temporal vein.
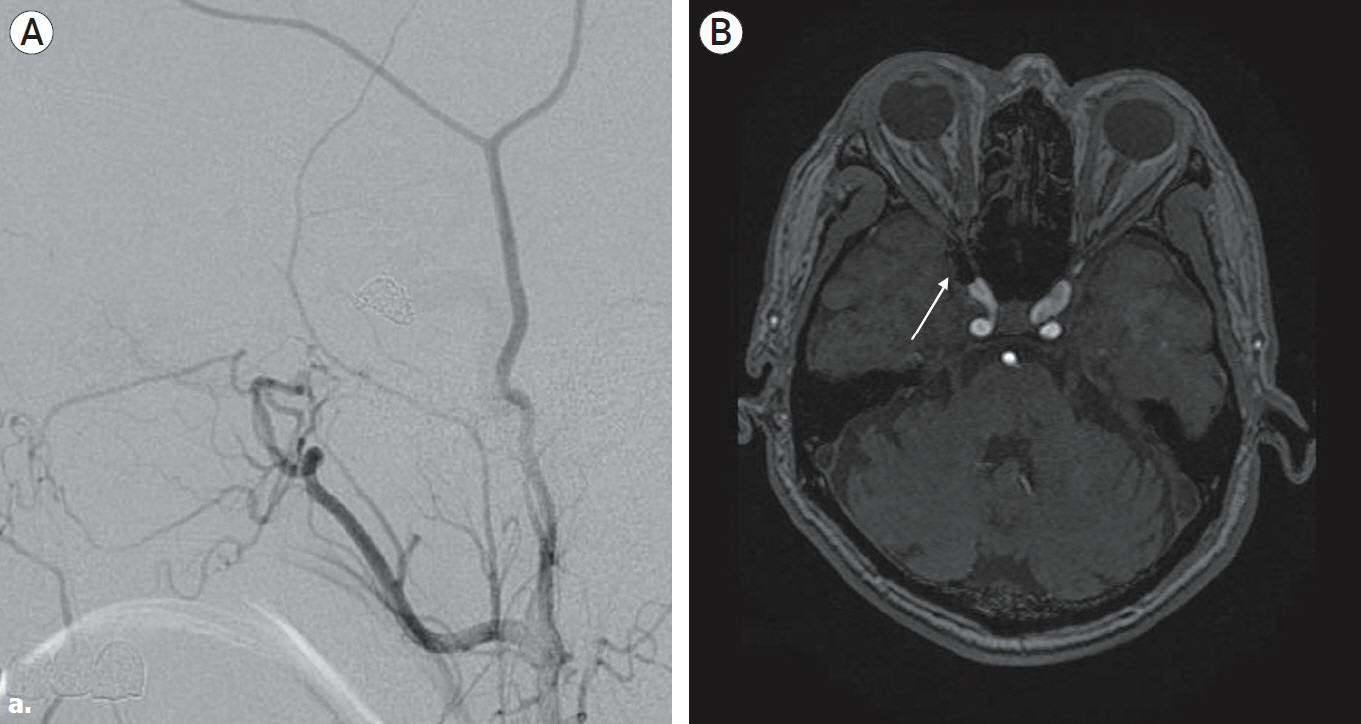
Fig. 4. Postoperative digital subtraction angiography (DSA) and magnetic resonance angiography. (A) The final DSA shows complete occlusion of the cavernous sinus dural arteriovenous fistula. (B) Axial magnetic resonance angiography source image shows coil (white arrow) in the right anterior cavernous sinus area.
Reference
-
1. Agid R, Willinsky RA, Haw C, Souza MPS, Vanek IJ, terBrugge KG. Targeted compartmental embolization of cavernous sinus dural arteriovenous fistulae using transfemoral medial and lateral facial vein approaches. Neuroradiology. 2004; Feb. 46(2):156–60.
Article2. Cheng KM, Chan CM, Cheung YL. Transvenous embolisation of dural carotid-cavernous fistulas by multiple venous routes: a series of 27 cases. Acta Neurochir (Wien). 2003; Jan. 145(1):17–29.
Article3. Devoto MH, Egbert JE, Tomsick TA, Kulwin DR. Acute exophthalmos during treatment of a cavernous sinus-dural fistula through the superior ophthalmic vein. Arch Ophthalmol. 1997; Jun. 115(6):823–4.
Article4. Dye J, Duckwiler G, Gonzalez N, Kaneko N, Goldberg R, Rootman D, et al. Endovascular approaches to the cavernous sinus in the setting of dural arteriovenous fistula. Brain Sci. 2020; Aug. 10(8):554.
Article5. Fattahi TT, Brandt MT, Jenkins WS, Steinberg B. Traumatic carotid-cavernous fistula: pathophysiology and treatment. J Craniofac Surg. 2003; Mar. 14(2):240–6.
Article6. Fu ZY, Feng Y, Ma C, Chen JC, Krings T, Zhao WY. Endovascular treatment of cavernous sinus dural arteriovenous fistulas via direct transorbital puncture using cone-beam computed tomography image guidance: report of 3 cases. World Neurosurg. 2019; Oct. 130:306–12.
Article7. Gemmete JJ, Ansari SA, Gandhi DM. Endovascular techniques for treatment of carotid-cavernous fistula. J Neuroophthalmol. 2009; Mar. 29(1):62–71.
Article8. Gupta N, Kikkawa DO, Levi L, Weinreb RN. Severe vision loss and neovascular glaucoma complicating superior ophthalmic vein approach to carotid-cavernous sinus fistula. Am J Ophthalmol. 1997; Dec. 124(6):853–5.
Article9. Halbach VV, Hieshima GB, Higashida RT, Reicher M. Carotid cavernous fistulae: indications for urgent treatment. AJR Am J Roentgenol. 1987; Sep. 149(3):587–93.
Article10. Han W, Kim JH, Kang HI, Kim DR, Moon BG, Kim JS. Transvenous embolization of dural carotid cavernous fistula through the supraorbital vein. J Cerebrovasc Endovasc Neurosurg. 2019; Jun. 21(2):101–6.
Article11. Henderson AD, Miller NR. Carotid-cavernous fistula: current concepts in aetiology, investigation, and management. Eye (Lond). 2018; Feb. 32(2):164–72.
Article12. Komiyama M, Morikawa K, Fu Y, Yagura H, Yasui T, Baba M. Indirect carotid-cavernous sinus fistula: transvenous embolization from the external jugular vein using a superior ophthalmic vein approach. A case report. Surg Neurol. 1990; Jan. 33(1):57–63.
Article13. Korkmazer B, Kocak B, Tureci E, Islak C, Kocer N, Kizilkilic O. Endovascular treatment of carotid cavernous sinus fistula: A systematic review. World J Radiol. 2013; Apr. 5(4):143–55.
Article14. Matsubara S, Kazekawa K, Aikawa H, Onizuka M, Tsutsumi M, Ikou M, et al. Direct superficial temporal vein approach for dural carotid cavernous fistula. Interv Neuroradiol. 2007; Mar. 13(Suppl 1):64–7.
Article15. Miller NR. Dural carotid-cavernous fistulas: epidemiology, clinical presentation, and management. Neurosurg Clin N Am. 2012; Jan. 23(1):179–92.
Article16. Miyachi S, Negoro M, Handa T, Sugita K. Dural carotid cavernous sinus fistula presenting as isolated oculomotor nerve palsy. Surg Neurol. 1993; Feb. 39(2):105–9.
Article17. Nokovitch L, Devauchelle B, Peyrachon B, Vacher C, Deneuve S. Anatomical characteristics of the superficial temporal venous system and implications in microsurgery. Ann Chir Plast Esthet. 2021; Jun. 66(3):250–6.18. Shimizu Y. Superficial middle temporal vein as a pivotal route to embolize dural carotid-cavernous fistulas. J Clin Neurosci. 2021; Feb. 84:106–10.
Article19. Singh J, Morris PP. Superficial temporal vein: route to embolization of cavernous dural arteriovenous fistula. J Neuroimaging. 2011; Jul. 21(3):251–4.
Article20. Suh DC, Lee JH, Kim SJ, Chung SJ, Choi CG, Kim HJ, et al. New concept in cavernous sinus dural arteriovenous fistula: correlation with presenting symptom and venous drainage patterns. Stroke. 2005; Jun. 36(6):1134–9.
Article21. Trivelato FP, Manzato LB, Filho PMM, Ulhoa AC, Vanzin JR, Abud DG, et al. Transorbital cavernous sinus direct puncture: Alternative to treat dural arteriovenous fistula. Clin Neuroradiol. 2018; Mar. 28(1):55–61.22. Yu SC, Cheng HK, Wong GK, Chan CM, Cheung JY, Poon WS. Transvenous embolization of dural carotid-cavernous fistulae with transfacial catheterization through the superior ophthalmic vein. Neurosurgery. 2007; Jun. 60(6):1032–7. discussion 1037-8.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Transvenous Embolization of Cavernous Sinus Dural Arteriovenous Fistula Using the Direct Superior Ophthalmic Vein Approach: A Case Report
- Facilitated Retrograde Access via the Facial Vein for Transvenous Embolization of the Cavernous Sinus Dural Arteriovenous Fistula with Isolated Ophthalmic Venous Drainage
- Transvenous Coil Embolization for Dural Arteriovenous Fistulas of the Ophthalmic Sheath: Report of Two Cases and Review of the Literature
- Transvenous injection of n-butyl 2-cyanoacrylate to obliterate the pathologic cavernous sinus as a salvage technique for incompletely obliterated complex cavernous sinus dural arteriovenous fistula after transvenous coil embolization
- Transvenous Embolization of Dural Carotid Cavernous Fistula through the Supraorbital Vein
