Biocreative Alveolar Molding Plate Treatment (BioAMP) for neonatal unilateral cleft lip and palate with excessively wide alveolar cleft and maxillary arch width
- Affiliations
-
- 1Department of Surgery, Division of Plastic and Reconstructive Surgery, Neonatal and Pediatric Craniofacial Airway Orthodontics, Stanford University School of Medicine, Lucile Packard Children’s Hospital Stanford, Palo Alto, CA, USA
- 2Department of Orthodontics, School of Dentistry, Kyung Hee University, Seoul, Korea
- KMID: 2551476
- DOI: http://doi.org/10.4041/kjod23.163
Abstract
- Since its inception in Europe in the 1950s, alveolar molding treatment for neonates with complete cleft lip and palate has undergone significant evolution in both design and application methodology, demonstrating effectiveness in normalizing the alveolar cleft and nasal shape. However, excessively wide alveolar clefts accompanied by disproportionately wide total maxillary arch pose significant challenges when utilizing conventional alveolar molding methods involving cyclical adding and grinding of acrylic on molding plates. The current report introduces a novel alveolar molding method named Biocreative Alveolar Molding Plate Treatment (BioAMP), which can normalize the maxillary alveolar cleft and arch shape without laborious conventional acrylic procedures. BioAMP sets the target arch form and provides unrestricted space for natural growth of the maxillary alveolar bones while systematically reducing the total maxillary arch width in precise increments. Two exemplary cases are presented as proofof-concept, showcasing the clinical innovation of BioAMP.
Keyword
Figure
-
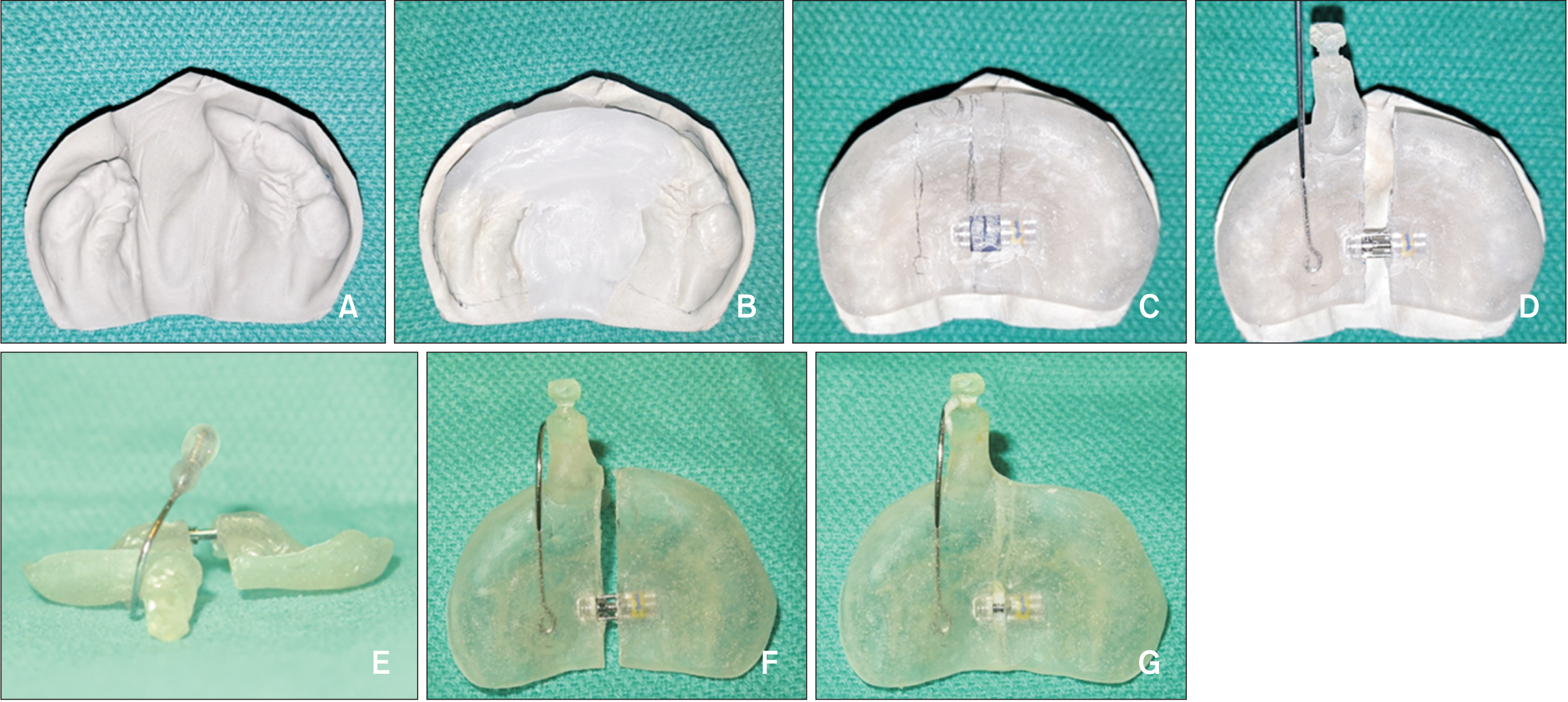
Figure 1 Biocreative Alveolar Molding Plate (BioAMP) with a constriction screw: Fabrication and implementation protocol. A, Occlusal view of a pre-treatment maxillary arch shape of a neonate with an excessively wide alveolar cleft accompanied by excessive total maxillary arch width. B, Wax-up for a target maxillary arch shape. C, Hard acrylic plate with a constriction screw in place. D, A button and nasal stent wire were installed prior to the delivery of the plate. The palatal plate is split in half to activate the constriction screw. E, Frontal view of the final form of the BioAMP after the nasal stent wire was fitted to the nasal dome inside the nose. The palatal plate remained split prior to activating the constriction screw. F, Occlusal view of the BioAMP after activating the constriction. G, Occlusal view of the BioAMP after the gap between the split halves was re-united using fresh hard acrylic. The total maxillary arch width is now less than before.
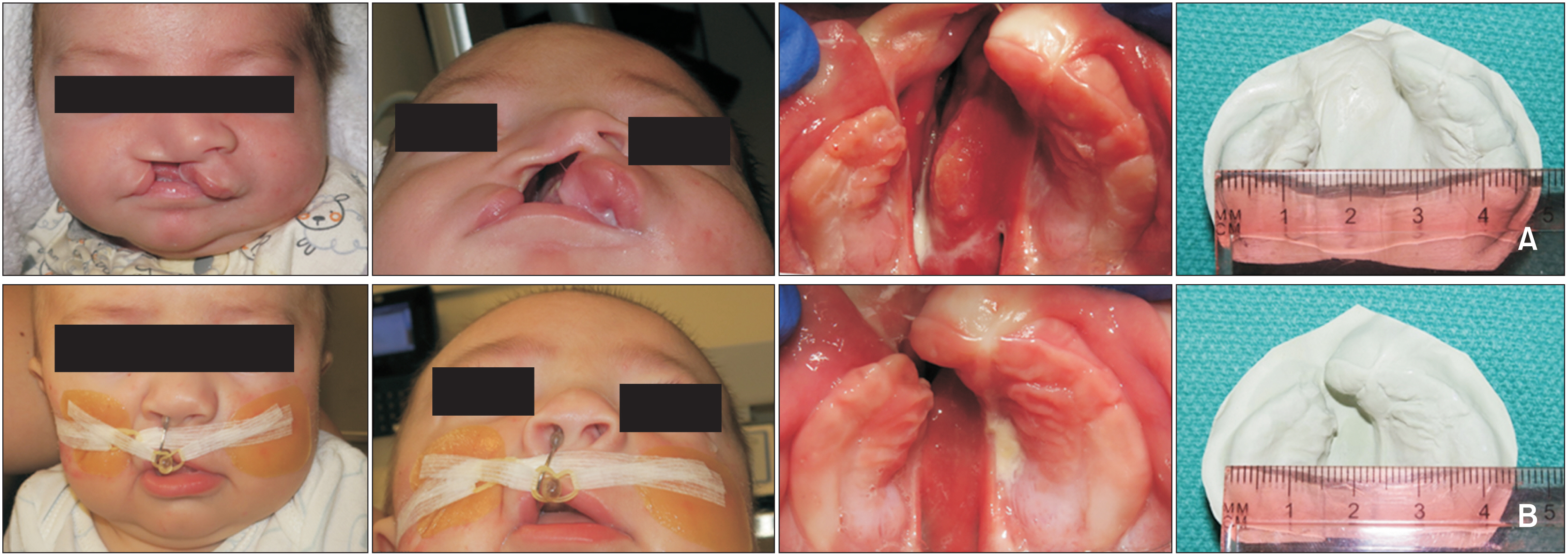
Figure 2 Patient 1 was treated with the BioAMP with a constriction screw. The images present the frontal facial view, wormʼs eye view, occlusal view of the maxillary arch, and a stone model of the maxillary arch (arranged from left to right): A, Pre-treatment at the age of 1 week. B, Post-treatment at the age of 2.5 months. The total maxillary arch width decreased from 47 to 42.5 mm, and the interalveolar gap decreased from 16 to 1 mm. Permission to use the photos was granted by the patientʼs parents.
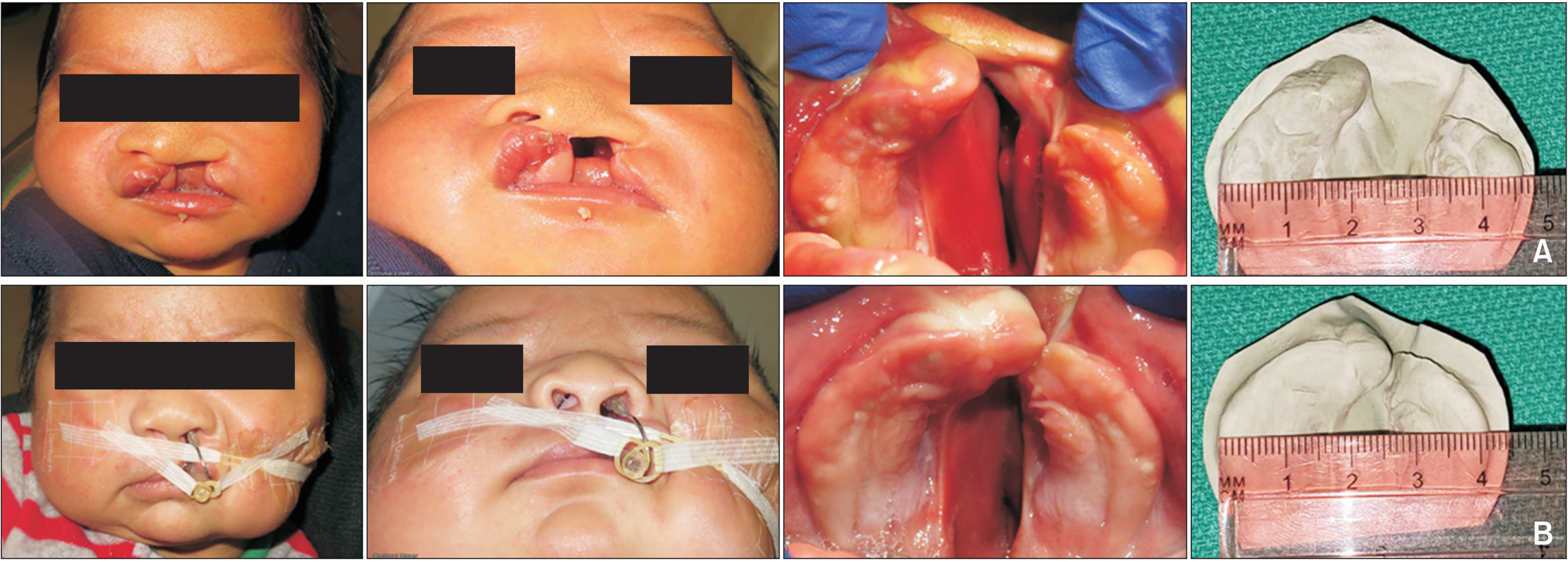
Figure 3 Patient 2 was treated with the BioAMP with a construction screw. The images present the frontal facial view, wormʼs eye view, occlusal view of the maxillary arch, and a stone model of the maxillary arch (arranged from left to right): A, Pre-treatment at the age of 2 weeks. B, Post-treatment at the age of 3 months. The total arch width decreased from 46 to 41 mm, and the interalveolar gap decreased from 15 to 0 mm. Permission to use the photos was granted by the patientʼs parents.
Reference
-
1. McNEIL CK. 1950; Orthodontic procedures in the treatment of congenital cleft palate. Dent Rec (London). 70:126–32. https://pubmed.ncbi.nlm.nih.gov/24537837/.2. Hotz M, Gnoinski W. 1976; Comprehensive care of cleft lip and palate children at Zürich university: a preliminary report. Am J Orthod. 70:481–504. https://doi.org/10.1016/0002-9416(76)90274-8. DOI: 10.1016/0002-9416(76)90274-8. PMID: 1068633.3. Matsuo K, Hirose T. 1988; Nonsurgical correction of cleft lip nasal deformity in the early neonate. Ann Acad Med Singap. 17:358–65. https://pubmed.ncbi.nlm.nih.gov/3064700/.4. Pool R, Farnworth TK. 1994; Preoperative lip taping in the cleft lip. Ann Plast Surg. 32:243–9. https://doi.org/10.1097/00000637-199403000-00003. DOI: 10.1097/00000637-199403000-00003. PMID: 8192382.5. Grayson BH, Santiago PE, Brecht LE, Cutting CB. 1999; Presurgical nasoalveolar molding in infants with cleft lip and palate. Cleft Palate Craniofac J. 36:486–98. https://doi.org/10.1597/1545-1569_1999_036_0486_pnmiiw_2.3.co_2. DOI: 10.1597/1545-1569_1999_036_0486_pnmiiw_2.3.co_2. PMID: 10574667.6. Clarren SK, Anderson B, Wolf LS. 1987; Feeding infants with cleft lip, cleft palate, or cleft lip and palate. Cleft Palate J. 24:244–9. https://pubmed.ncbi.nlm.nih.gov/3477346/.7. Mak SY, Wong WH, Or CK, Poon AM. 2006; Incidence and cluster occurrence of palatal fistula after furlow palatoplasty by a single surgeon. Ann Plast Surg. 57:55–9. https://doi.org/10.1097/01.sap.0000205176.90736.e4. DOI: 10.1097/01.sap.0000205176.90736.e4. PMID: 16799309.8. Choo H, Maguire M, Low DW. 2012; Modified technique of presurgical infant maxillary orthopedics for complete unilateral cleft lip and palate. Plast Reconstr Surg. 129:249–52. https://doi.org/10.1097/PRS.0b013e318230c8bb. DOI: 10.1097/PRS.0b013e318230c8bb. PMID: 22186514.9. Bauer FX, Güll FD, Roth M, Ritschl LM, Rau A, Gau D, et al. 2017; A prospective longitudinal study of postnatal dentoalveolar and palatal growth: the anatomical basis for CAD/CAM-assisted production of cleft-lip-palate feeding plates. Clin Anat. 30:846–54. https://doi.org/10.1002/ca.22892. DOI: 10.1002/ca.22892. PMID: 28459132.10. Tankittiwat P, Pisek A, Manosudprasit M, Punyavong P, Manosudprasit A, Phaoseree N, et al. 2021; Function of nasoalveolar molding devices in bilateral complete cleft lip and palate: a 3-dimensional maxillary arch analysis. Cleft Palate Craniofac J. 58:1389–97. https://doi.org/10.1177/1055665621990184. DOI: 10.1177/1055665621990184. PMID: 33657892.11. Bhutiani N, Tripathi T, Rai P. 2022; Active nasoalveolar molding using 3-directional expansion screw for arch alignment in bilateral cleft lip and palate. AJO-DO Clin Companion. 2:20–5. https://doi.org/10.1016/j.xaor.2021.12.003. DOI: 10.1016/j.xaor.2021.12.003.12. Suri S, Disthaporn S, Atenafu EG, Fisher DM. 2012; Presurgical presentation of columellar features, nostril anatomy, and alveolar alignment in bilateral cleft lip and palate after infant orthopedics with and without nasoalveolar molding. Cleft Palate Craniofac J. 49:314–24. https://doi.org/10.1597/10-204. DOI: 10.1597/10-204. PMID: 21981581.13. Zheng J, He H, Kuang W, Yuan W. 2019; Presurgical nasoalveolar molding with 3D printing for a patient with unilateral cleft lip, alveolus, and palate. Am J Orthod Dentofacial Orthop. 156:412–9. https://doi.org/10.1016/j.ajodo.2018.04.031. DOI: 10.1016/j.ajodo.2018.04.031. PMID: 31474271.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Unilateral Complete Cleft Lip and Palate Repair Using Lip Adhesion and Passive Alveolar Molding Appliance: Effect on the Maxillary Alveolar Arch
- Three-dimensional evaluation of alveolar changes induced by nasoalveolar molding in infants with unilateral cleft lip and palate: A case-control study
- Presurgical naso-alveolar molding appliance for unilateral cleft lip and palate
- Effect of Presurgical Orthopedics and Lip Adhesion on Maxillary Alveolar Arch in Complete Unilateral Cleft of Primary and Secondary Palate
- A study on the maxillary dental arch and palate of unilateral cleft lip and palate individuals
