Three-dimensional evaluation of alveolar changes induced by nasoalveolar molding in infants with unilateral cleft lip and palate: A case-control study
- Affiliations
-
- 1Private Practice, Istanbul, Turkey.
- 2Department of Orthodontics, Faculty of Dentistry, Yeditepe University, Istanbul, Turkey. dgermec@gmail.com
- KMID: 2458617
- DOI: http://doi.org/10.4041/kjod.2019.49.5.286
Abstract
OBJECTIVE
The objectives of this study were to evaluate linear and volumetric alveolar changes induced by nasoalveolar molding (NAM) in infants with complete unilateral cleft lip and palate (UCLP) and compare the maxillary dimensions after NAM with the normal dimensions in infants without clefts.
METHODS
A total of 26 infants with UCLP treated by NAM (mean age before and after NAM: 14.20 ± 8.09 days and 118.16 ± 10.06 days, respectively) comprised the treatment group, while 26 infants without clefts (mean age: 115.81 ± 8.71 days) comprised the control group. Changes in the maxillary dimensions following NAM were measured on three-dimensional models using Mimics software, version 17.0.
RESULTS
During NAM, there was a decrease in the cleft widths, maxillary arch depths, and rotation of the greater segment. While the anterior alveolar arch width exhibited a significant decrease, the posterior arch width was mostly maintained. There were no changes in the anterior vertical deviations of the alveolar segments. The alveolar crest lengths, arch circumference, and bilateral posterior volumetric measures exhibited an increase. After NAM, the anterior arch width was comparable between the treatment and control groups, whereas the posterior arch width and anterior vertical deviations were greater in the treatment group than in the control group. The maxillary arch depths, alveolar crest lengths, and maxillary volumes were smaller in the NAM group than in the control group.
CONCLUSIONS
During NAM in infants with UCLP, the cleft width and anteroposterior and transverse alveolar dimensions exhibited a decrease while the vertical dimensions were maintained. Compared with infants without clefts, those with UCLP treated by NAM exhibited sagittal and vertical alveolar growth deficiencies and tissue insufficiency.
Keyword
Figure
-

Figure 1 Positioning of landmarks for the measurement of alveolar changes after nasoalveolar molding in infants with unilateral cleft lip and palate. A, The landmarks are positioned on a maxillary virtual model using Mimics software, version 17.0 (Materialise, Leuven, Belgium). After positioning on the three-dimensional model, the location of each landmark (in this figure, B point) was two-dimensionally checked in the axial, sagittal, and coronal planes. B, For evaluation of the vertical deviations, a horizontal plane is constructed using the following three points: 1) greater segment tuberosity point (T), 2) lesser segment tuberosity point (T′), and 3) greater segment canine point (C2). See Table 1 for definitions of each landmark.
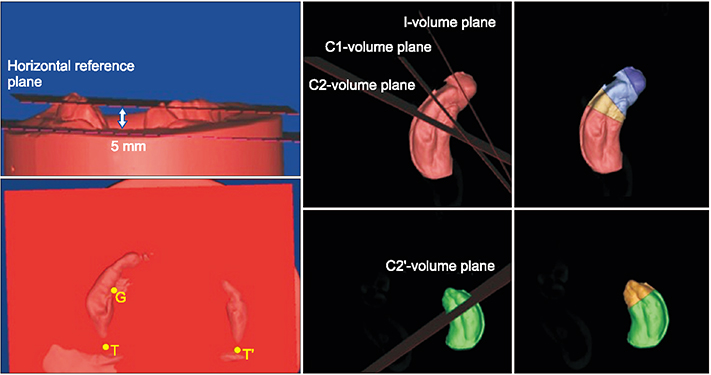
Figure 2 Alveolar segmentation for the measurement of changes after nasoalveolar molding in infants with unilateral cleft lip and palate. The alveolar segments are separated from the maxillary virtual model 5 mm below the horizontal reference plane. For volumetric measurements, the segments are sectioned using the I, C1, C2, and C2′ volumetric planes. See Table 1 for definitions of each landmark.
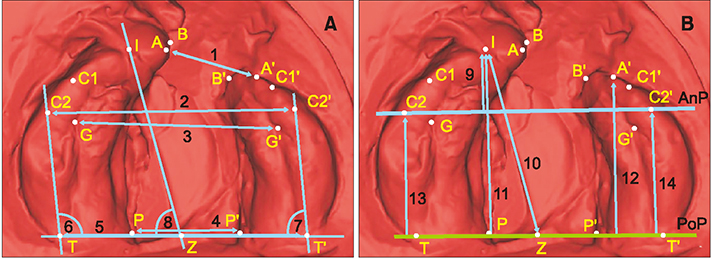
Figure 3 Transverse and sagittal measurements after nasoalveolar molding in infants with unilateral cleft lip and palate. A, Transverse linear and angular measurements. B, Sagittal measurements. 1, Anterior cleft width (A-A′); 2, anterior arch width (C2-C2′); 3, inferior anterior arch width (G-G′); 4, posterior cleft width (P-P′); 5, posterior arch width (T-T′); 6, posterior position of the greater segment (Z-T-C2); 7, posterior position of the lesser segment (Z-T′-C2′); 8, greater segment rotation (I-Z-T); 9, anterior arch depth (I-AnP); 10, anterior position of the greater segment (I-Z); 11, total arch depth (I-PoP); 12, alveolar arch length in the lesser segment (A′-PoP); 13, canine-posterior plane distance in the greater segment (C2-PoP); 14, canine-posterior plane distance in the lesser segment (C2′-PoP).
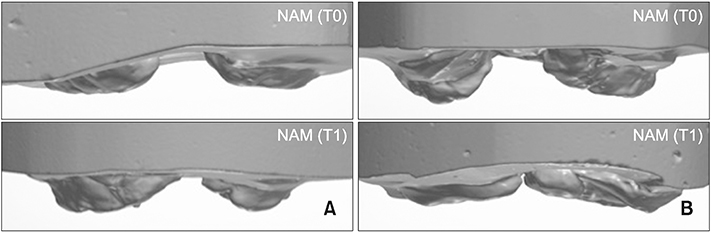
Figure 4 Vertical deviations after nasoalveolar molding (NAM) in two different representative cases with unilateral cleft lip and palate. A, Increased vertical deviations after treatment. In this patient, the initial vertical deviations did not improve with treatment, probably because of the excessive vertical component of the extraoral force caused by inappropriate use of the retention tapes or individual differences in the amount of tissue deficiency and growth potential. B, Decreased vertical deviations after treatment. In this patient, a significant decrease has occurred as a result of vertical trimming inside the appliance and growth during the treatment. T0, Before treatment; T1, after treatment.
Reference
-
1. Grayson BH, Cutting C, Wood R. Preoperative columella lengthening in bilateral cleft lip and palate. Plast Reconstr Surg. 1993; 92:1422–1423.2. Grayson BH, Santiago PE, Brecht LE, Cutting CB. Presurgical nasoalveolar molding in infants with cleft lip and palate. Cleft Palate Craniofac J. 1999; 36:486–498.
Article3. Grayson BH, Cutting CB. Presurgical nasoalveolar orthopedic molding in primary correction of the nose, lip, and alveolus of infants born with unilateral and bilateral clefts. Cleft Palate Craniofac J. 2001; 38:193–198.
Article4. Kriens O. Data-objective diagnosis of infant cleft lip, alveolus, and palate. Morphologic data guiding understanding and treatment concepts. Cleft Palate Craniofac J. 1991; 28:157–168.
Article5. Mazaheri M, Athanasiou AE, Long RE Jr, Kolokitha OG. Evaluation of maxillary dental arch form in unilateral clefts of lip, alveolus, and palate from one month to four years. Cleft Palate Craniofac J. 1993; 30:90–93.
Article6. Berkowitz S. Facial and palatal growth. In : Berkowitz S, editor. Cleft lip and palate. 2nd ed. Heidelberg: Springer;2006. p. 23–34.7. Huddart AG, MacCauley FJ, Davis ME. Maxillary arch dimensions in normal and unilateral cleft palate subjects. Cleft Palate J. 1969; 6:471–487.8. Mishima K, Sugahara T, Mori Y, Sakuda M. Three-dimensional comparison between the palatal forms in infants with complete unilateral cleft lip, alveolus, and palate (UCLP) with and without Hotz's plate. Cleft Palate Craniofac J. 1996; 33:77–83.
Article9. Wada T, Miyazaki T. Growth and changes in maxillary arch form in complete unilateral cleft lip and cleft palate children. Cleft Palate J. 1975; 12:115–130.10. Bacher M, Göz G, Pham T, Bacher U, Werner O, Buchner P, et al. Three-dimensional analysis of cleft palate topology in newborn infants with reference to the cranial skeleton. Cleft Palate Craniofac J. 1998; 35:379–395.
Article11. Baek SH, Son WS. Difference in alveolar molding effect and growth in the cleft segments: 3-dimensional analysis of unilateral cleft lip and palate patients. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006; 102:160–168.
Article12. Ezzat CF, Chavarria C, Teichgraeber JF, Chen JW, Stratmann RG, Gateno J, et al. Presurgical nasoalveolar molding therapy for the treatment of unilateral cleft lip and palate: a preliminary study. Cleft Palate Craniofac J. 2007; 44:8–12.
Article13. Yağcı A, Uysal T. Evaluation of the effects of nasoalveolar molding method on cleft segments and alveolar widths of babies with unilateral cleft lip and palate. Sağlık Bilimleri Dergisi. 2007; 16:1–10.14. Keçik D, Enacar A. Effects of nasoalveolar molding therapy on nasal and alveolar morphology in unilateral cleft lip and palate. J Craniofac Surg. 2009; 20:2075–2080.
Article15. Sabarinath VP, Thombare P, Hazarey PV, Radhakrishnan V, Agrekar S. Changes in maxillary alveolar morphology with nasoalveolar molding. J Clin Pediatr Dent. 2010; 35:207–212.
Article16. Yu Q, Gong X, Shen G. CAD presurgical nasoalveolar molding effects on the maxillary morphology in infants with UCLP. Oral Surg Oral Med Oral Pathol Oral Radiol. 2013; 116:418–426.
Article17. Mandwe RS, Puri S, Shingane S, Pawar G, Kolhe VR, Alsi A. Presurgical nasoalveolar remodeling - an experience in the journey of cleft lip and palate. Clin Cosmet Investig Dent. 2015; 7:1–7.18. Börnert H, Dannhauer KH, Schmalzried D. Vertical changes in the positions of the cleft segments of patients with unilateral cleft lip and palate. Changes from birth to palatoplasty at the age of 10–14 months. J Orofac Orthop. 2002; 63:51–61.
Article19. Grayson BH, Maull D. Nasoalveolar molding for infants born with clefts of the lip, alveolus and palate. In : Berkowitz S, editor. Cleft lip and palate. 2nd ed. Heidelberg: Springer;2006. p. 451–458.20. Braumann B, Keilig L, Stellzig-Eisenhauer A, Bourauel C, Bergé S, Jäger A. Patterns of maxillary alveolar arch growth changes of infants with unilateral cleft lip and palate: preliminary findings. Cleft Palate Craniofac J. 2003; 40:363–372.
Article21. Isogawa N, Ochiai S, Mito T, Kindaichi J, Ishibashi N, Takagi Y, et al. Three-dimensional comparison in palatal forms between modified presurgical nasoalveolar molding plate and Hotz's plate applied to the infants with unilateral cleft lip and palate. Singapore Dent J. 2010; 31:36–42.
Article22. Hotz MM, Gnoinski WM. Effects of early maxillary orthopaedics in coordination with delayed surgery for cleft lip and palate. J Maxillofac Surg. 1979; 7:201–210.
Article23. Millard DR Jr, Latham RA. Improved primary surgical and dental treatment of clefts. Plast Reconstr Surg. 1990; 86:856–871.
Article24. Adali N, Mars M, Petrie A, Noar J, Sommerlad B. Presurgical orthopedics has no effect on archform in unilateral cleft lip and palate. Cleft Palate Craniofac J. 2012; 49:5–13.
Article25. Prahl C, Kuijpers-Jagtman AM, Van't Hof MA, Prahl-Andersen B. A randomized prospective clinical trial of the effect of infant orthopedics in unilateral cleft lip and palate: prevention of collapse of the alveolar segments (Dutchcleft). Cleft Palate Craniofac J. 2003; 40:337–342.
Article26. Berkowitz S, Duncan R, Evans C, Friede H, Kuijpers-Jagtman AM, Prahl-Anderson B, et al. Timing of cleft palate closure should be based on the ratio of the area of the cleft to that of the palatal segments and not on age alone. Plast Reconstr Surg. 2005; 115:1483–1499.
Article27. Burston WR. The early orthodontic treatment of cleft palate conditions. Dent Pract. 1958; 9:41–52.28. Huddart AG. Presurgical changes in unilateral cleft palate subjects. Cleft Palate J. 1979; 16:147–157.29. Braumann B, Rosenhayn SE, Bourauel C, Jäger A. Two- or three-dimensional cast analysis in patients with cleft lip and palate? J Orofac Orthop. 2001; 62:451–465.
Article30. Berkowitz S. The effect of clefting of the lip and palate an the palatal arch form. In : Berkowitz S, editor. Cleft lip and palate. 2nd ed. Heidelberg: Springer;2006. p. 43–54.31. Braumann B, Keilig L, Bourauel C, Jäger A. Three-dimensional analysis of morphological changes in the maxilla of patients with cleft lip and palate. Cleft Palate Craniofac J. 2002; 39:1–11.
Article32. Wada T, Mizokawa N, Miyazaki T, Ergen G. Maxillary dental arch growth in different types of cleft. Cleft Palate J. 1984; 21:180–192.33. Sillman JH. Dimensional changes of the dental arches: longitudinal study from birth to 25 years. Am J Orthod. 1964; 50:824–842.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Effect of presurgical nasoalveolar molding (PNAM) appliance and cheiloplasty on alveolar molding of complete unilateral cleft lip and palate patients
- Presurgical naso-alveolar molding appliance for unilateral cleft lip and palate
- Comparative evaluation of nasal and alveolar changes in complete unilateral cleft lip and palate patients using intraoral and extraoral nasoalveolar molding techniques: randomized controlled trial
- Biocreative Alveolar Molding Plate Treatment (BioAMP) for neonatal unilateral cleft lip and palate with excessively wide alveolar cleft and maxillary arch width
- Correction of Unilateral Cleft Lip Using Surgeon-Made Nasoalveolar Molding Device
