Xanthogranulomatous inflammation of the lower jaw bone: a rare case report
- Affiliations
-
- 1Department of Oral and Maxillofacial Surgery, Sun Dental Hospital, Daejeon, Korea
- 2Department of Oral and Maxillofacial Surgery, Daejeon Sun Hospital, Daejeon, Korea
- KMID: 2550300
- DOI: http://doi.org/10.5125/jkaoms.2023.49.6.360
Abstract
- Xanthogranulomatous inflammation (XGI) is an uncommon type of chronic inflammation and is histologically characterized by foamy histiocytes and giant cells. The most common sites of occurrence are kidneys and gallbladder. The etiology remains controversial. Involvement of the lower jaw bone is rare. In this study, we report a case of XGI presenting in the lower jaw.
Figure
-
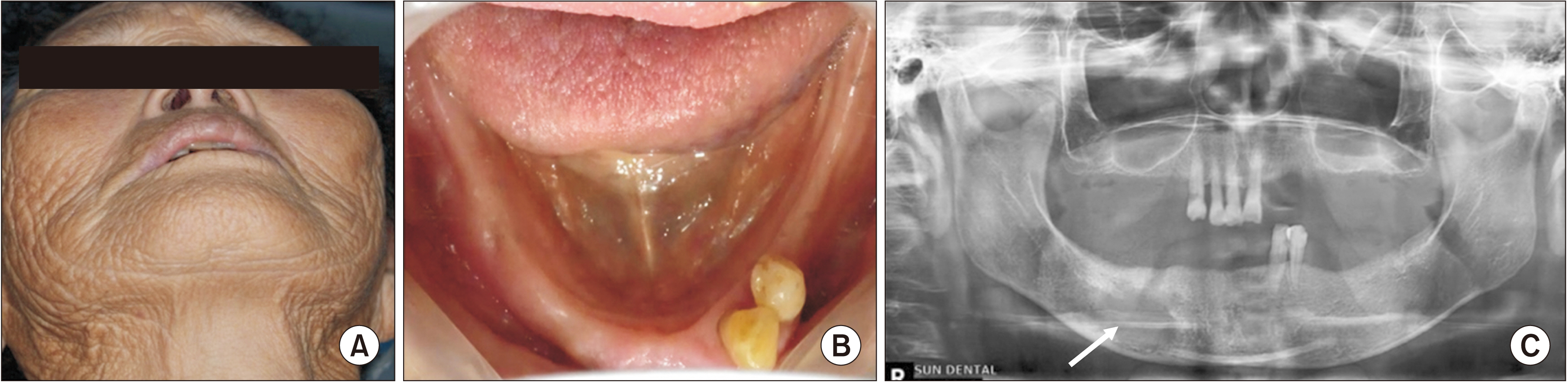
Fig. 1 Preoperative photographs and X-ray. A. No facial swelling and redness on the right body of the mandible. B. Gingival swelling on the right body of the mandible and a fistula tract in the #44 extraction area. C. A radiolucent lesion was observed on X-ray (panorama) imaging (arrow).
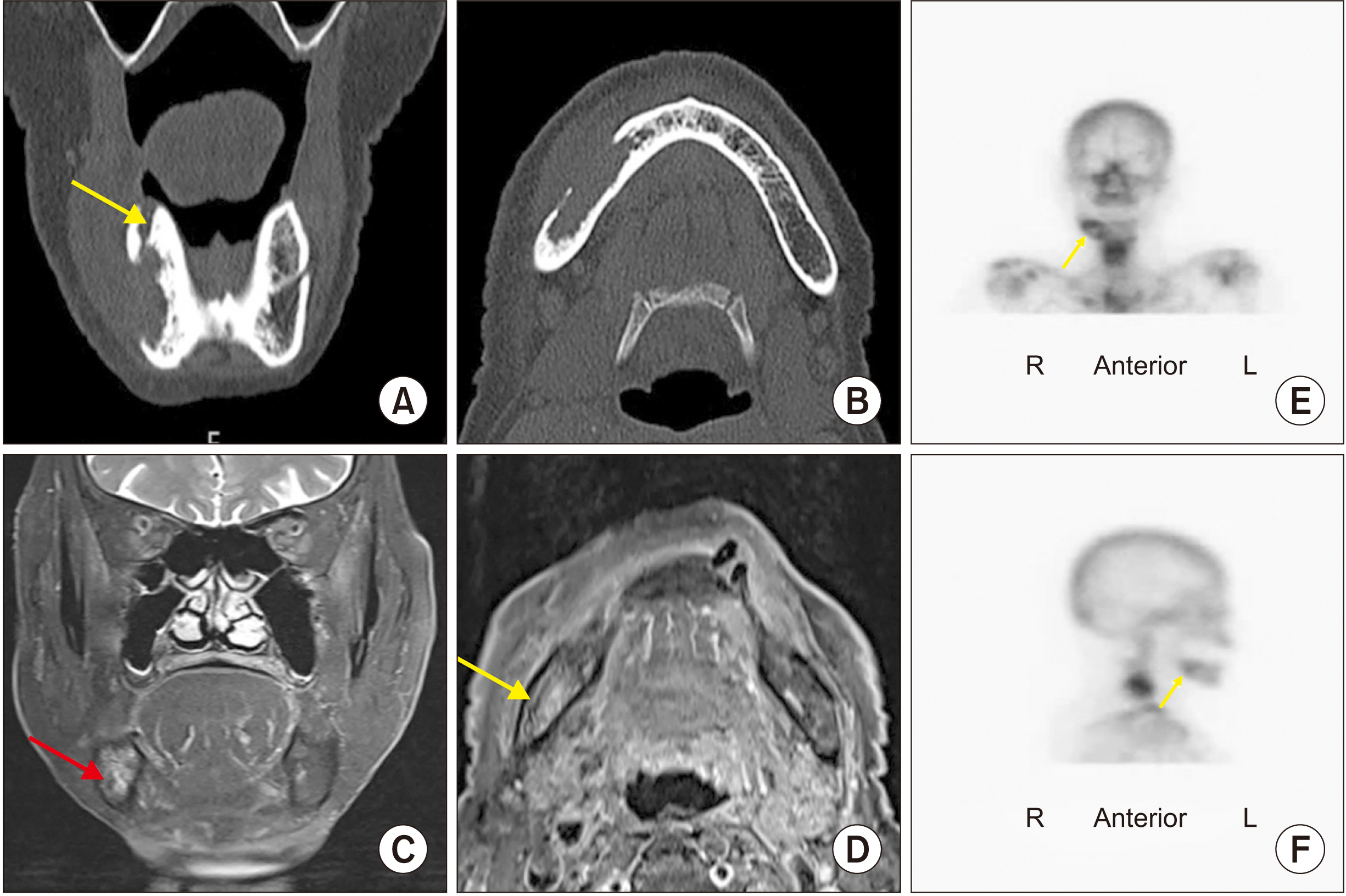
Fig. 2 Preoperative computed tomography (CT), magnetic resonance imaging (MRI), and 3-phase bone scan. A. On CT images, a fistula tract was observed in the #44 extracted region (yellow arrow). B. Bony resorption was noted. C, D. MRI imaging revealed an intraosseous lesion displaying high intensity. The right inferior alveolar nerve (red arrow) was involved in the mass (yellow arrow). E, F. A focal hot spot was observed on the right body of the mandible (yellow arrows).

Fig. 3 Surgical procedure. A, B. A crestal incision was created, and a mucoperiosteal flap was elevated to expose the bone and mass. C. A releasing incision around the mental nerve was completed with a #15 blade. D. The mental nerve was dissected from the mass. E. Retrograde dissection of the mental nerve was initiated to identify the inferior alveolar nerve (IAN) anterior to the mass. F. A subsequent anterograde dissection was performed. G. The mass was separated from the IAN. H. The IAN was repositioned to the inferior mandibular border. Guardix-SG (sodium hyaluronate, HA; Hanmi Pharm.), CMC (sodium carboxymethylcellulose; Hanmi Pharm.), and P-STOP (collagen; Ecott Co.) were applied to the IAN to prevent adhesion with the bone graft materials. I. Graft bone (xenograft, bone substitute cancellous granules; Purgo Biologics) material was used to graft the site.

Fig. 4 The excised mass specimen. A 4-cm-sized, irregularly margined, hard, yellowish mass.
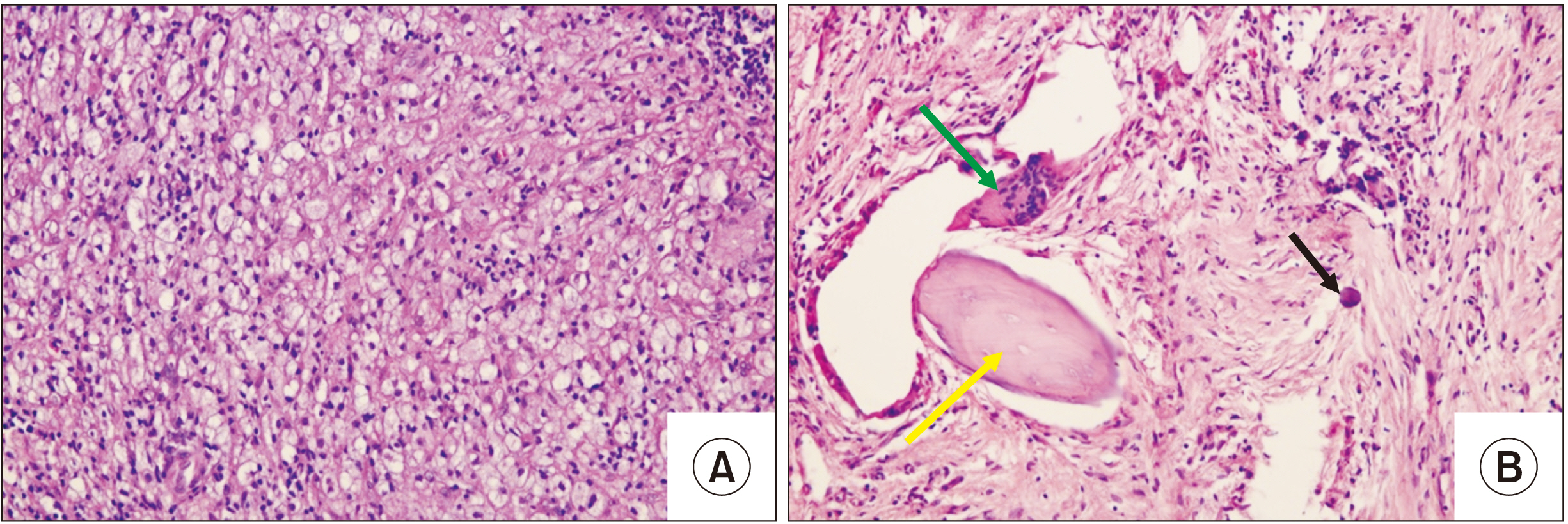
Fig. 5 A. Foam cells. B. Necrotic bone (yellow arrow), histocytes (green arrow), and fibrosis (black arrow). H&E staining (A, B: ×200).
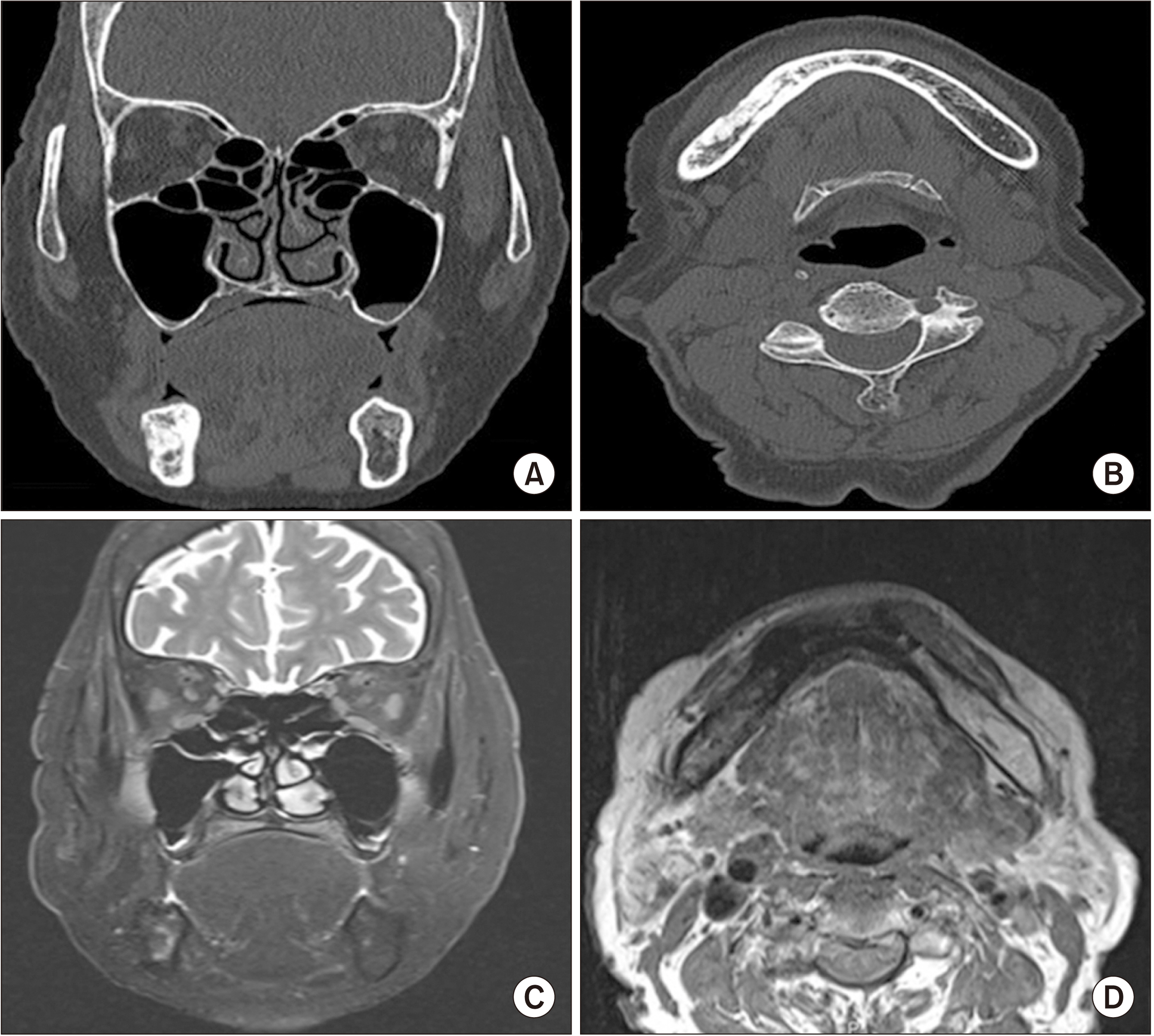
Fig. 6 Postoperative 9 months computed tomography (CT) and magnetic resonance imaging (MRI). The fistula tract was healed, there was no recurrence (A, C), and the bone at the operation site was regenerated (B, D) on CT and MRI images at postoperative 9 months.
Reference
-
References
1. Nomura T, Momose S, Takashima M, Kikuchi S. 2019; A case of neck xanthogranulomatous inflammation-suspected malignant tumor. Clin Case Rep. 7:1323–6. https://doi.org/10.1002/ccr3.2220. DOI: 10.1002/ccr3.2220. PMID: 31360477. PMCID: PMC6637363.2. Lee SH, Lee YH, Park H, Cho YJ, Song HT, Yang WI, et al. 2013; A case report of xanthogranulomatous osteomyelitis of the distal ulna mimicking a malignant neoplasm. Am J Case Rep. 14:304–7. https://doi.org/10.12659/ajcr.889422. DOI: 10.12659/AJCR.889422. PMID: 23961304. PMCID: PMC3745271.3. Solooki S, Hoveidaei AH, Kardeh B, Azarpira N, Salehi E. 2019; Xanthogranulomatous osteomyelitis of the tibia. Ochsner J. 19:276–81. https://doi.org/10.31486/toj.18.0165. DOI: 10.31486/toj.18.0165. PMID: 31528142. PMCID: PMC6735604.4. Cozzutto C, Carbone A. 1988; The xanthogranulomatous process. Xanthogranulomatous inflammation. Pathol Res Pract. 183:395–402. https://doi.org/10.1016/s0344-0338(88)80085-2. DOI: 10.1016/S0344-0338(88)80085-2. PMID: 3054826.5. Krishna M, Dayal S. 2021; Xanthogranulomatus inflammatory lesion mimicker of malignancy: a clinicopathological study from rural India. North Clin Istanb. 8:485–92. https://doi.org/10.14744/nci.2021.04317. DOI: 10.14744/nci.2021.04317. PMID: 34909587. PMCID: PMC8630717.6. Taskin OC, Gucer H, Winer D, Mete O. 2015; Thyroglossal duct cyst associated with xanthogranulomatous inflammation. Head Neck Pathol. 9:530–3. https://doi.org/10.1007/s12105-015-0628-y. DOI: 10.1007/s12105-015-0628-y. PMID: 25896144. PMCID: PMC4651935.7. Mehdinezhad-Kashani M, Zarif-Zakerian B, Shayan K, Riyasi F. 2010; Xanthogranulomatous osteomyelitis of femur: report of one case. Iran J Orthop Surg. 8:187–90.8. Cheema A, Arkader A, Pawel B. 2017; Xanthogranulomatous osteomyelitis of the humerus in a pediatric patient with Alagille syndrome: a case report and literature review. Skeletal Radiol. 46:1447–52. https://doi.org/10.1007/s00256-017-2707-5. DOI: 10.1007/s00256-017-2707-5. PMID: 28660405.9. Rawal YB, Chandra SR, Hall JM. 2017; Central xanthoma of the jaw bones: a benign tumor. Head Neck Pathol. 11:192–202. https://doi.org/10.1007/s12105-016-0764-z. DOI: 10.1007/s12105-016-0764-z. PMID: 27771838. PMCID: PMC5429282.10. Shimokata H, Kuzuya F. 1995; Two-point discrimination test of the skin as an index of sensory aging. Gerontology. 41:267–72. https://doi.org/10.1159/000213693. DOI: 10.1159/000213693. PMID: 8537010.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Cecal Cancer with Xanthogranulomatous Inflammation
- Focal Xanthogranulomatous Pyelonephritis Associated with Xanthogranulomatous Cholecystitis: A Case Report
- A Case of Xanthogranulomatous Pyelonephritis Associated with Xanthogranulomatous Epididymoorchitis
- Xanthogranulomatous Epididymitis
- A Case of Gossypiboma Associated with Xanthogranulomatous Inflammation
