Ann Rehabil Med.
2023 Dec;47(6):519-527. 10.5535/arm.23056.
Association Between Mobilization Level And Activity of Daily Living Independence in Critically Ill Patients
- Affiliations
-
- 1Department of Rehabilitation, National Hospital Organization, Nagoya Medical Center, Nagoya, Japan
- 2Department of Physical Therapy, Faculty of Rehabilitation, Gifu University of Health Science, Gifu, Japan
- 3Critical Care Research Group, The Prince Charles Hospital, Chermside, Australia
- 4Department of Cardiopulmonary Rehabilitation Science, Nagasaki University Graduate School of Biomedical Sciences, Nagasaki, Japan
- 5Department of Rehabilitation, Naha City Hospital, Naha, Japan
- 6Department of Healthcare Administration, The University of Kyushu, Fukuoka, Japan
- 7Department of rehabilitation, Steel Memorial Yawata Hospital, Kitakyushu, Japan
- 8Japanese Society for Early Mobilization, Tokyo, Japan
- 9Department of Critical Care Medicine, National Hospital Organization, Nagoya Medical Center, Nagoya, Japan
- KMID: 2549733
- DOI: http://doi.org/10.5535/arm.23056
Abstract
Objective
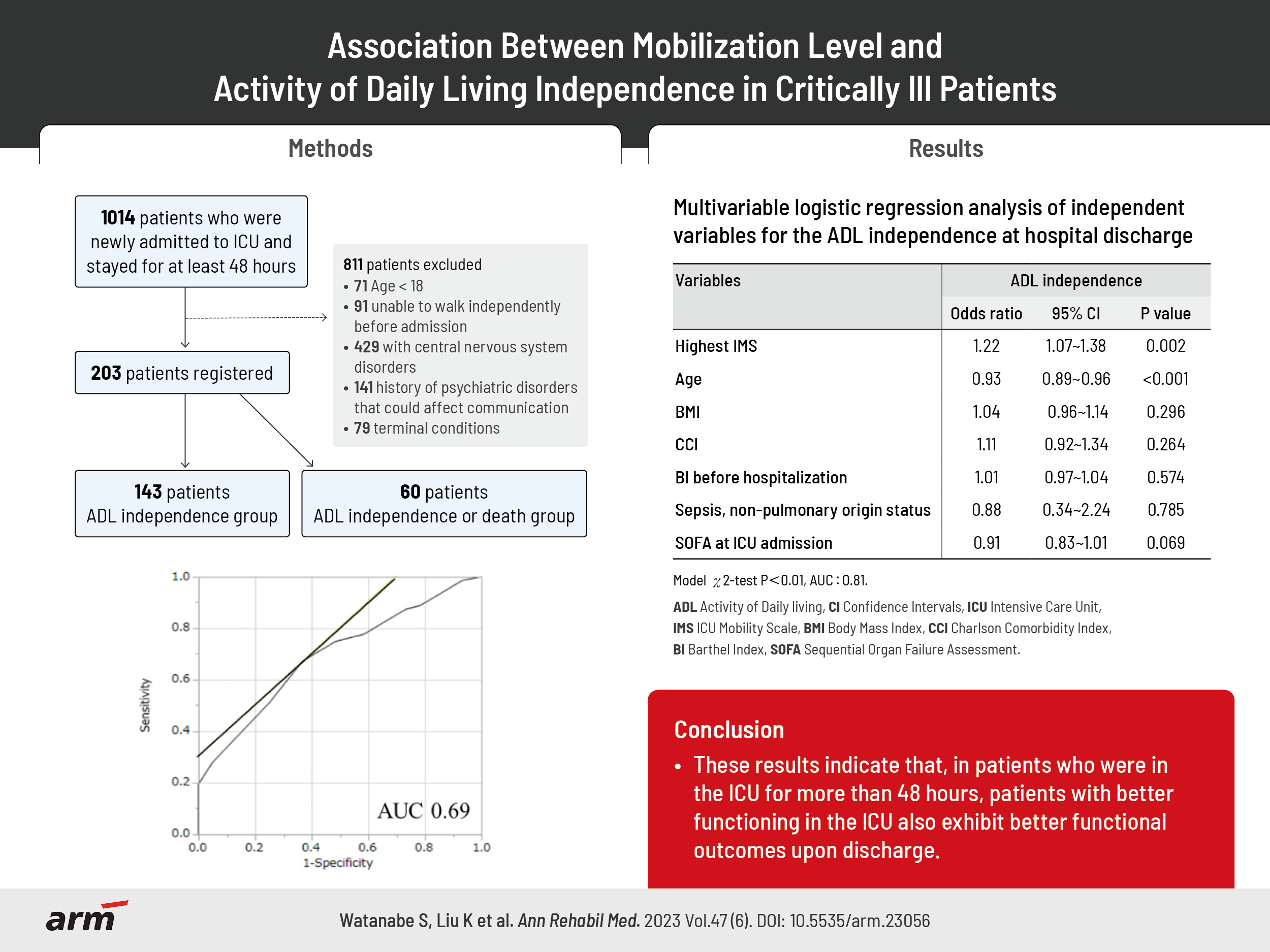
To examine the association between the mobilization level during intensive care unit (ICU) admission and independence in activity of daily living (ADL), defined as Barthel Index (BI)≥70.
Methods
This was a post-hoc analysis of the EMPICS study involving nine hospitals. Consecutive patients who spend >48 hours in the ICU were eligible for inclusion. Mobilization was performed at each hospital according to the shared protocol and the highest ICU mobility score (IMS) during the ICU stay, baseline characteristics, and BI at hospital discharge. Multiple logistic regression analysis, adjusted for baseline characteristics, was used to deter-mine the association between the highest IMS (using the receiver operating characteristic [ROC]) and ADL.
Results
Of the 203 patients, 143 were assigned to the ADL independence group and 60 to the ADL dependence group. The highest IMS score was significantly higher in the ADL independence group than in the dependence group and was a predictor of ADL independence at hospital discharge (odds ratio, 1.22; 95% confidence interval, 1.07–1.38; adjusted p=0.002). The ROC cutoff value for the highest IMS was 6 (specificity, 0.67; sensitivity, 0.70; area under the curve, 0.69).
Conclusion
These results indicate that, in patients who were in the ICU for more than 48 hours, that patients with good function in the ICU also exhibit good function upon discharge. However, prospective, multicenter trials are needed to confirm this conclusion.
Keyword
Figure
-

Fig. 1. Flow chart of the patient selection process. ICU, intensive care unit; ADL, activity of daily living.

Fig. 2. Receiver operating characteristic curve for highest intensive care unit mobility scale and independence of activity daily living. AUC, area under the curve.
Reference
-
1. Needham DM, Davidson J, Cohen H, Hopkins RO, Weinert C, Wunsch H, et al. Improving long-term outcomes after discharge from intensive care unit: report from a stakeholders' conference. Crit Care Med. 2012; 40:502–9.2. Myers EA, Smith DA, Allen SR, Kaplan LJ. Post-ICU syndrome: rescuing the undiagnosed. JAAPA. 2016; 29:34–7.3. Ad Hoc Committee for Early Rehabilitation; The Japanese Society of Intensive Care Medicine. [Evidence based expert consensus for early rehabilitation in the intensive care unit]. J Jpn Soc Intensive Care Med. 2017; 24:255–303. Japanese.4. Tipping CJ, Harrold M, Holland A, Romero L, Nisbet T, Hodgson CL. The effects of active mobilisation and rehabilitation in ICU on mortality and function: a systematic review. Intensive Care Med. 2017; 43:171–83.
Article5. Watanabe S, Iida Y, Ito T, Mizutani M, Morita Y, Suzuki S, et al. Effect of early rehabilitation activity time on critically ill patients with intensive care unit-acquired weakness: a Japanese retrospective multicenter study. Prog Rehabil Med. 2018; 3:20180003.
Article6. Nishida O, Ogura H, Egi M, Fujishima S, Hayashi Y, Iba T, et al. The Japanese Clinical Practice Guidelines for Management of Sepsis and Septic Shock 2016 (J-SSCG 2016). Acute Med Surg. 2018; 5:3–89.7. Schweickert WD, Pohlman MC, Pohlman AS, Nigos C, Pawlik AJ, Esbrook CL, et al. Early physical and occupational therapy in mechanically ventilated, critically ill patients: a randomised controlled trial. Lancet. 2009; 373:1874–82.
Article8. Kayambu G, Boots R, Paratz J. Physical therapy for the critically ill in the ICU: a systematic review and meta-analysis. Crit Care Med. 2013; 41:1543–54.9. Watanabe S, Liu K, Morita Y, Kanaya T, Naito Y, Suzuki S, et al. Effects of mobilization among critically ill patients in the intensive care unit: a single-center retrospective study. Prog Rehabil Med. 2022; 7:20220013.10. Morris PE, Goad A, Thompson C, Taylor K, Harry B, Passmore L, et al. Early intensive care unit mobility therapy in the treatment of acute respiratory failure. Crit Care Med. 2008; 36:2238–43.
Article11. Watanabe S, Liu K, Nakamura K, Kozu R, Horibe T, Ishii K, et al. Association between early mobilization in the ICU and psychiatric symptoms after surviving a critical illness: a multi-center prospective cohort study. J Clin Med. 2022; 11:2587.
Article12. Watanabe S, Morita Y, Suzuki S, Kochi K, Ohno M, Liu K, et al. Effects of the intensity and activity time of early rehabilitation on activities of daily living dependence in mechanically ventilated patients. Prog Rehabil Med. 2021; 6:20210054.
Article13. Tymkew H, Norris T, Arroyo C, Schallom M. the use of physical therapy ICU assessments to predict discharge home. Crit Care Med. 2020; 48:1312–8.
Article14. Denehy L, Lanphere J, Needham DM. Ten reasons why ICU patients should be mobilized early. Intensive Care Med. 2017; 43:86–90.
Article15. Katsukawa H, Ota K, Liu K, Morita Y, Watanabe S, Sato K, et al. Risk factors of patient-related safety events during active mobilization for intubated patients in intensive care units-a multi-center retrospective observational study. J Clin Med. 2021; 10:2607.
Article16. Watanabe S, Kotani T, Taito S, Ota K, Ishii K, Ono M, et al. Determinants of gait independence after mechanical ventilation in the intensive care unit: a Japanese multicenter retrospective exploratory cohort study. J Intensive Care. 2019; 7:53.
Article17. Hodgson C, Needham D, Haines K, Bailey M, Ward A, Harrold M, et al. Feasibility and inter-rater reliability of the ICU Mobility Scale. Heart Lung. 2014; 43:19–24. Erratum in: Heart Lung 2014;43:388.
Article18. Shiroiwa T, Ikeda S, Noto S, Igarashi A, Fukuda T, Saito S, et al. Comparison of value set based on DCE and/or TTO data: scoring for EQ-5D-5L health states in Japan. Value Health. 2016; 19:648–54.
Article19. Watanabe S, Liu K, Morita Y, Kanaya T, Naito Y, Arakawa R, et al. Changes in barriers to implementing early mobilization in the intensive care unit: a single center retrospective cohort study. Nagoya J Med Sci. 2021; 83:443–64.20. Harrold ME, Salisbury LG, Webb SA, Allison GT; Australia and Scotland ICU Physiotherapy Collaboration. Early mobilisation in intensive care units in Australia and Scotland: a prospective, observational cohort study examining mobilisation practises and barriers. Crit Car. 2015; 19:336.
Article21. Patel BK, Pohlman AS, Hall JB, Kress JP. Impact of early mobilization on glycemic control and ICU-acquired weakness in critically ill patients who are mechanically ventilated. Chest. 2014; 146:583–9.
Article22. Stephens MA. EDF statistics for goodness of fit and some comparisons. J Am Stat Assoc. 1974; 69:730–7.
Article23. Huang M, Chan KS, Zanni JM, Parry SM, Neto SG, Neto JA, et al. Functional Status Score for the ICU: an international clinimetric analysis of validity, responsiveness, and minimal important difference. Crit Care Med. 2016; 44:e1155–64.
Article24. Denehy L, de Morton NA, Skinner EH, Edbrooke L, Haines K, Warrillow S, et al. A physical function test for use in the intensive care unit: validity, responsiveness, and predictive utility of the physical function ICU test (scored). Phys Ther. 2013; 93:1636–45.
Article25. Hermans G, Clerckx B, Vanhullebusch T, Segers J, Vanpee G, Robbeets C, et al. Interobserver agreement of Medical Research Council sum-score and handgrip strength in the intensive care unit. Muscle Nerve. 2012; 45:18–25.
Article26. Thrush A, Rozek M, Dekerlegand JL. The clinical utility of the functional status score for the intensive care unit (FSS-ICU) at a long-term acute care hospital: a prospective cohort study. Phys Ther. 2012; 92:1536–45. Erratum in: Phys Ther 2013;93:282.
Article27. Skinner EH, Berney S, Warrillow S, Denehy L. Development of a physical function outcome measure (PFIT) and a pilot exercise training protocol for use in intensive care. Crit Care Resusc. 2009; 11:110–5.
Article28. Nydahl P, Wilkens S, Glase S, Mohr LM, Richter P, Klarmann S, et al. The German translation of the Perme Intensive Care Unit Mobility Score and inter-rater reliability between physiotherapists and nurses. Eur J Physiother. 2017; 20:109–15.
Article29. Tipping CJ, Bailey MJ, Bellomo R, Berney S, Buhr H, Denehy L, et al. The ICU mobility scale has construct and predictive validity and is responsive. A multicenter observational study. Ann Am Thorac Soc. 2016; 13:887–93.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Sedation in the Critically Ill Patients
- Effects of Active Vibration Exercise on Trunk Muscle Activity, Balance, and Activities of Daily Living in Patients with Chronic Stroke
- A Study on the Stress of Family-Caregivers and Level of Daily Living Performance with Patients of Cerebra Vascular Accident(CVA)
- A Study on Satisfaction with Care Service depending on Activities of Daily Living and Type of Caregivers among Inpatients with Chronic Disease
- The Relationship Between Activity Daily Living and Powerlessness of Spinal Cord Injury Patient's
