Group B Streptococcus meningitis following subarachnoid hemorrhage suspicions: a case report
- Affiliations
-
- 1Department Anesthesiology and Perioperative Medicine, Virginia Commonwealth University School of Medicine, Richmond, VA, USA
- KMID: 2549489
- DOI: http://doi.org/10.18700/jnc.230028
Abstract
- Background
Bacterial meningitis is a life-threatening disease associated with high morbidity and mortality. Subarachnoid hemorrhage (SAH) can accompany bacterial meningitis in adult patients in <1% of cases and significantly worsens the patient’s prognosis.
Case report
A 58-year-old man presented to the emergency department complaining of a 5-day history of progressive abdominal pain, when he suddenly developed “the worst headache of his life” and suffered a 4-minute seizure. Computed tomography head showed SAH. An emergent cerebral angiogram was negative for any bleeding source, and attention shifted to meningoencephalitis. Ultimately, the patient was found to have Group B Streptococcus (GBS) meningitis on cerebrospinal fluid polymerase chain reaction.
Conclusion
To the best of our knowledge, this patient’s presentation of GBS meningitis, masked by a classic aneurysmal SAH presentation, represents a rare and acute presentation of an underlying disease complication. Increasing awareness of this presentation can support more rapid diagnosis, earlier treatment, and improved outcomes for affected patients.
Keyword
Figure
-
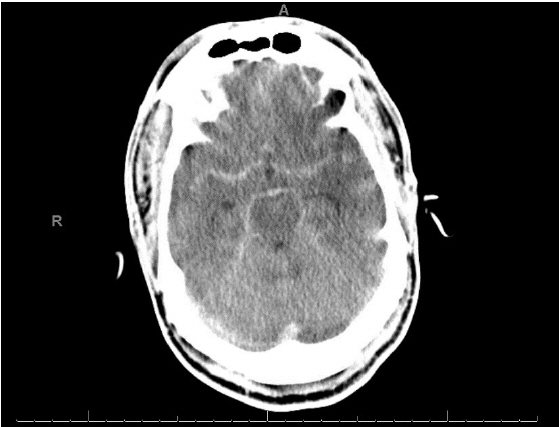
Fig. 1. Non-contrast head computed tomography demonstrating increased enhancement throughout most of the subarachnoid space, suggestive of meningoencephalitis or subarachnoid hemorrhage.

Fig. 2. Digital subtraction angiography performed the day of presentation. (A) Right internal carotid artery shows absence of vascular malformations including aneurysms. (B) Left internal carotid artery shows absence of vascular malformations including aneurysms. (C) Posterior circulation as seen also found to have no vascular malformations including aneurysms.

Fig. 3. Magnetic resonance imaging with and without intravenous contrast. (A) Evidence of diffusion restriction indicative of ischemia from EP2D sequence. Additional pus material with restriction effusion layering at the posterior horns of lateral ventricles. (B) Apparent diffusion coefficient (ADC) correlate of the same level as panel (A) demonstrating persistent diffusion restriction from EP2D ADC sequence. (C) Evidence of increased fluid-attenuated inversion recovery signal with association enhancement suggestive of diffuse meningitis.
Reference
-
1. van de Beek D, Brouwer MC, Koedel U, Wall EC. Community-acquired bacterial meningitis. Lancet. 2021; 398:1171–83.2. Al-Bayati A, Douedi S, Alsaoudi G, Mosseri M, Albustani S, Upadhyaya V, et al. Meningitis from invasive Streptococcus agalactiae in a healthy young adult. IDCases. 2020; 21:e00907.3. Deliran SS, Brouwer MC, van de Beek D. Subarachnoid hemorrhage in bacterial meningitis patients. Cerebrovasc Dis. 2022; 51:118–24.4. Kannoth S, Iyer R, Thomas SV, Furtado SV, Rajesh BJ, Kesavadas C, et al. Intracranial infectious aneurysm: presentation, management and outcome. J Neurol Sci. 2007; 256:3–9.5. Mook-Kanamori BB, Fritz D, Brouwer MC, van der Ende A, van de Beek D. Intracerebral hemorrhages in adults with community associated bacterial meningitis in adults: should we reconsider anticoagulant therapy? PLoS One. 2012; 7:e45271.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Intracerebral Thrombosis and Cortical Hemorrhage Complicated by Streptococcus pneumoniae Meningitis
- Streptococcus viridans Meningitis After Epidural Nerve Block
- Two Cases of Cerebral Infarctions Complicated by Streptococcus pneumoniae Meningitis
- A Case of Bilateral Endogenous Endophthalmitis in a Streptococcus pneumoniae Meningitis Patient
- Spontaneous Spinal Subarachnoid Hemorrhage Report of a Case
