Case of Concomitant Endoscopic Treatment of Achalasia with Superficial Esophageal Cancer
- Affiliations
-
- 1Department of Internal Medicine, Kosin University College of Medicine, Busan, Korea
- KMID: 2548495
- DOI: http://doi.org/10.4166/kjg.2023.099
Abstract
- Achalasia, a rare motility disorder of the esophagus, is generally accepted as a premalignant disorder. This paper presents the case of a 72-year-old male with achalasia and synchronous superficial esophageal cancer who experienced dysphagia symptoms for five years. As achalasia is associated with an increased risk of esophageal cancer, both can be treated simultaneously if detected at the time of diagnosis. Achalasia and synchronous esophageal cancer are rarely detected and treated endoscopically. This paper reports a case of concurrent successful treatment.
Figure
-
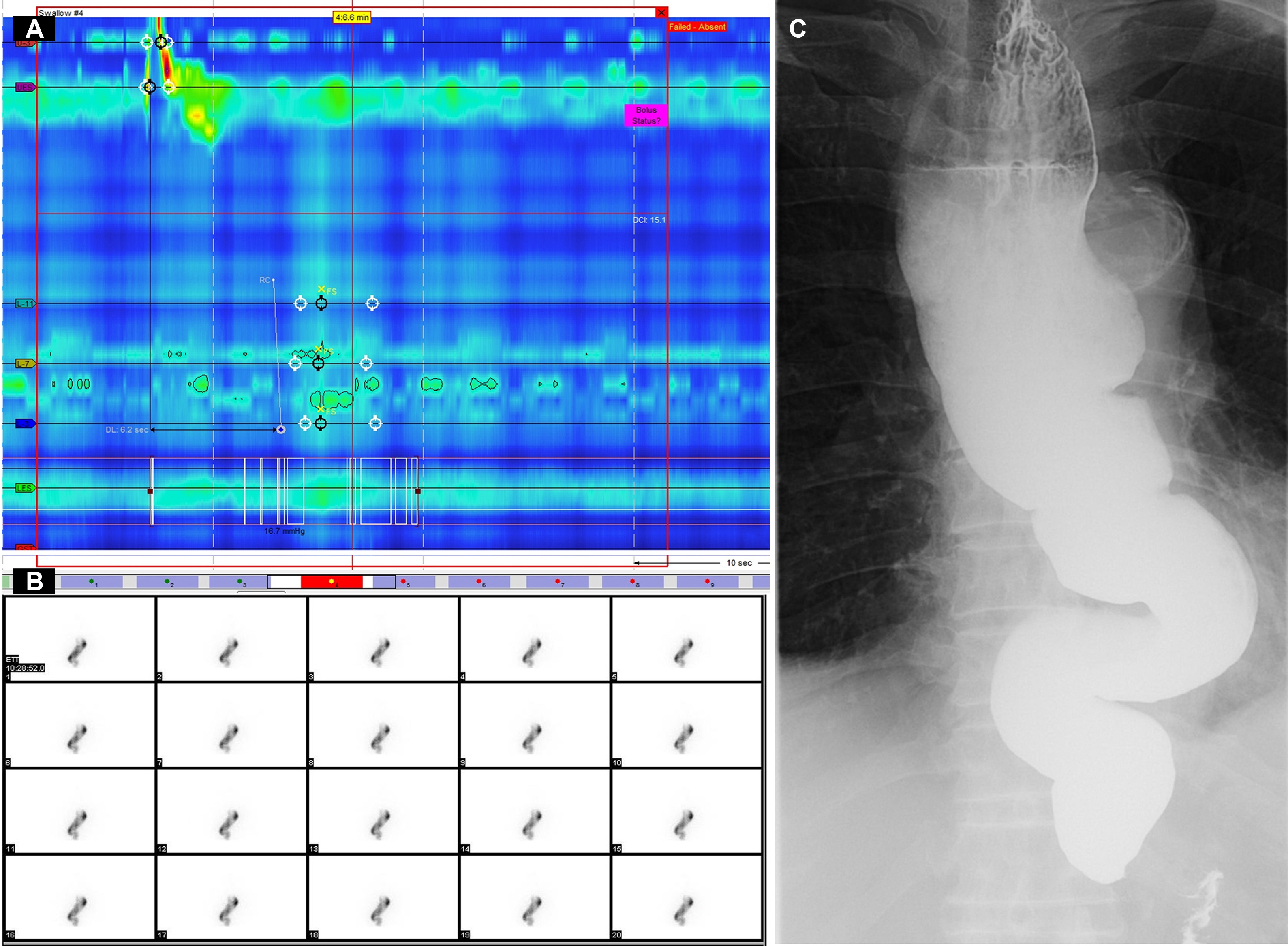
Fig. 1 Pre-procedure studies. (A) High-resonance manometry (HRM). HRM indicated type I achalasia owing to the absence of peristalsis, no contractile activity, and no pressurization within the esophageal body. (B) Dynamic esophageal scintigraphy showing prolongation of esophageal transit time. (C) Barium esophagography reveals a “bird-beak” appearance of the esophagogastric junction, with a dilated esophageal body and sigmoid-like appearance.
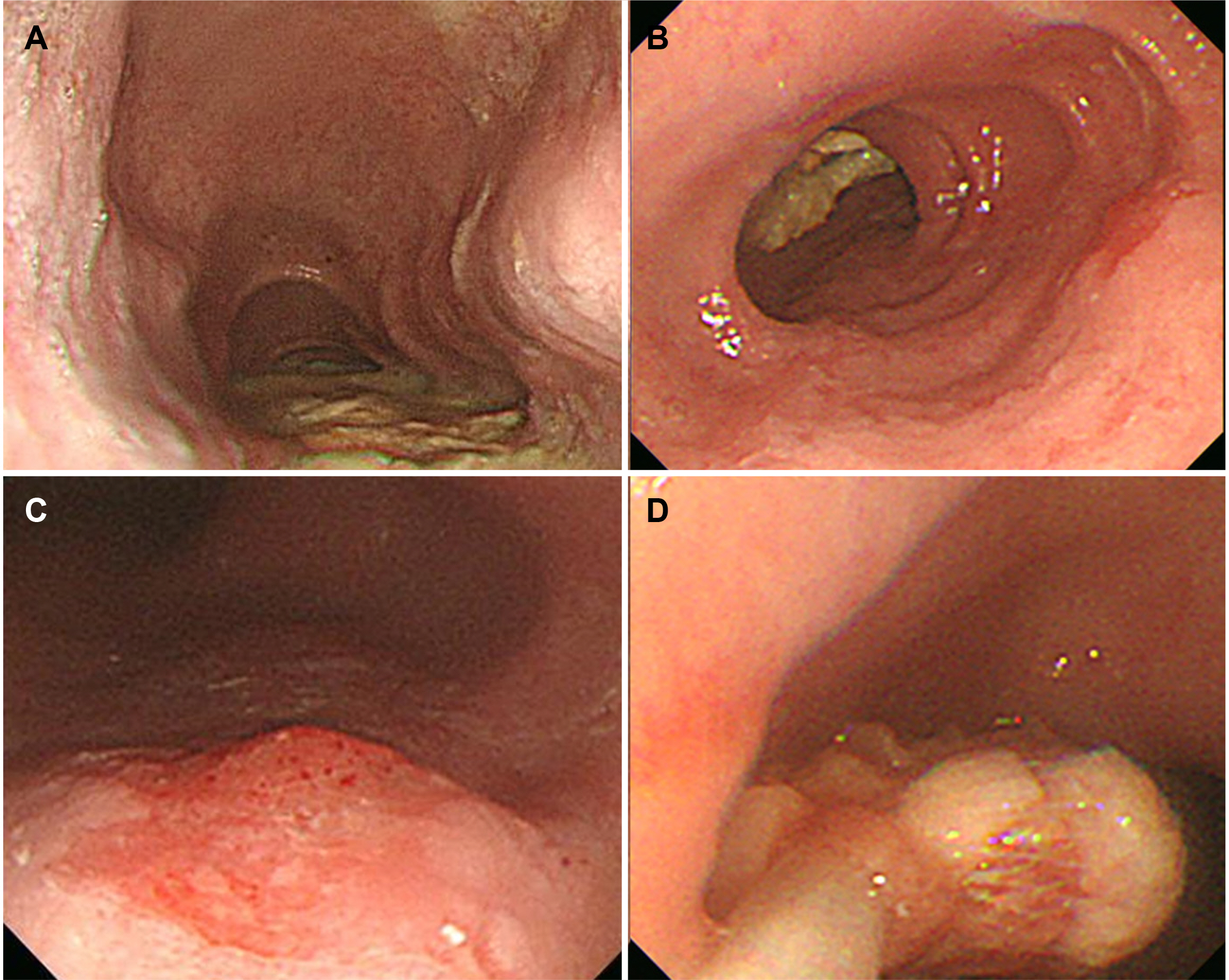
Fig. 2 Endoscopic findings. (A) Dilated esophagus drooping to both sides of the spine. (B) The narrowing of the distal esophagus is noted with food retention. (C) A 15 mm sized, hyperemic depressed lesion with vascular abnormality suspicious for esophageal cancer is observed 33 cm from the upper incisor. (D) Endoscopic food residue removal was performed.

Fig. 3 Endoscopic submucosal dissection (ESD) for esophageal superficial cancer. (A) White light image view of the lesion. (B) The narrow banding image endoscopy revealed a demarcated line, indicating the lesion margins as a brownish area. (C) The lesion was evaluated using Lugol’s solution (iodine), revealing no iodine uptake. (D) After marking and pre-cut, submucosal dissection was performed. (E) En-bloc resection was achieved, and the post-ESD scar was present on endoscopy.

Fig. 4 Peroral endoscopic myotomy for achalasia. (A) and (B) mucosal injections. (C) A submucosal tunnel is established. (D) The submucosa is dissected distally along the muscular layer. (E) Myotomy is performed. (F) The mucosal entry was closed with clipping.
Reference
-
1. Vaezi MF, Pandolfino JE, Vela MF. 2013; ACG clinical guideline: diagnosis and management of achalasia. Am J Gastroenterol. 108:1238–1249. quiz 1250DOI: 10.1038/ajg.2013.196. PMID: 23877351.
Article2. Fagge CH. 1872; A case of simple stenosis of the oesophagus, followed by epithelioma. Guy's Hosp Report (London). 17:413.3. Sato H, Terai S, Shimamura Y, et al. 2021; Achalasia and esophageal cancer: a large database analysis in Japan. J Gastroenterol. 56:360–370. DOI: 10.1007/s00535-021-01763-6. PMID: 33538893.
Article4. Leeuwenburgh I, Haringsma J, Van Dekken H, Scholten P, Siersema PD, Kuipers EJ. Long-term risk of oesophagitis, Barrett's oesophagus and oesophageal cancer in achalasia patients. Scand J Gastroenterol Suppl. 2006; (243):7–10. DOI: 10.1080/00365520600664201. PMID: 16782616.
Article5. Sato H, Nishikawa Y, Abe H, et al. 2022; Esophageal carcinoma in achalasia patients managed with endoscopic submucosal dissection and peroral endoscopic myotomy: Japan Achalasia Multicenter Study. Dig Endosc. 34:965–973. DOI: 10.1111/den.14197. PMID: 34787940.
Article6. Ghoshal UC, Daschakraborty SB, Singh R. 2012; Pathogenesis of achalasia cardia. World J Gastroenterol. 18:3050–3057. DOI: 10.3748/wjg.v18.i24.3050. PMID: 22791940. PMCID: PMC3386318.
Article7. Jung HK, Hong SJ, Lee OY, et al. 2020; 2019 Seoul consensus on esophageal achalasia guidelines. J Neurogastroenterol Motil. 26:180–203. DOI: 10.5056/jnm20014. PMID: 32235027. PMCID: PMC7176504.
Article8. Aadam AA, Abe S. 2018; Endoscopic submucosal dissection for superficial esophageal cancer. Dis Esophagus. 31:doy021. DOI: 10.1093/dote/doy021. PMID: 29982386.
Article9. Das A, Singh V, Fleischer DE, Sharma VK. 2008; A comparison of endoscopic treatment and surgery in early esophageal cancer: an analysis of surveillance epidemiology and end results data. Am J Gastroenterol. 103:1340–1345. DOI: 10.1111/j.1572-0241.2008.01889.x. PMID: 18510606.
Article10. Tang X, Ren Y, Jiang B, Gong W. 2015; Education and imaging: Gastroenterology: Endoscopic mucosal resection for esophageal dysplasia in an achalasia patient followed by peroral endoscopic myotomy. J Gastroenterol Hepatol. 30:1563. DOI: 10.1111/jgh.13034. PMID: 26177680.
Article11. Shi S, Fu K, Dong XQ, Hao YJ, Li SL. 2017; Combination of concurrent endoscopic submucosal dissection and modified peroral endoscopic myotomy for an achalasia patient with synchronous early esophageal neoplasms. World J Gastrointest Endosc. 9:99–104. DOI: 10.4253/wjge.v9.i2.99. PMID: 28250904. PMCID: PMC5311480.
Article12. Park JC, Lee YC, Kim SK, et al. 2009; Achalasia combined with esophageal cancer treated by concurrent chemoradiation therapy. Gut Liver. 3:329–333. DOI: 10.5009/gnl.2009.3.4.329. PMID: 20431771. PMCID: PMC2852741.
Article13. Goudra B, Saumoy M. 2022; Anesthesia for advanced endoscopic procedures. Clin Endosc. 55:1–7. DOI: 10.5946/ce.2021.236. PMID: 34974678. PMCID: PMC8831399.14. Leeuwenburgh I, Scholten P, Alderliesten J, et al. 2010; Long-term esophageal cancer risk in patients with primary achalasia: a prospective study. Am J Gastroenterol. 105:2144–2149. DOI: 10.1038/ajg.2010.263. PMID: 20588263.
Article15. Han SY, Youn YH. 2023; Role of endoscopy in patients with achalasia. Clin Endosc. 56:537–545. DOI: 10.5946/ce.2023.001. PMID: 37430397. PMCID: PMC10565433.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Role of endoscopy in patients with achalasia
- A Case of Esophageal Carcinoma Following Esophagomyotomy for Achalasia
- Endoscopic Treatment of Primary Esophageal Motility Disorders
- Peroral Endoscopic Myotomy for Esophageal Motility Disorders
- Non-achalasia esophageal motility disorders: Role of per-oral endoscopic myotomy
