Calcium channel blockers for hypertension: old, but still useful
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Wonkwang University Sanbon Hospital, Gunpo, Korea
- KMID: 2547302
- DOI: http://doi.org/10.36011/cpp.2023.5.e16
Abstract
- Calcium channel blockers (CCBs) constitute a heterogeneous class of drugs that can be divided into dihydropyridines (DHPs) and non-DHPs. DHP-CCBs are subcategorized into four generations based on the duration of activity and pharmacokinetics, while non-DHP-CCBs are subcategorized into phenylethylamine and benzodiazepine derivatives. DHP-CCBs are vascular-selective and function as potent vasodilators, whereas non-DHP-CCBs are cardiac-selective and are useful for treating tachyarrhythmia, but reduce cardiac contractility and heart rate. Traditional DHP-CCBs (nifedipine) mainly block L-type calcium channels, whereas novel CCBs block N-type (amlodipine) and/or T-type channels (efonidipine) in addition to L-type channels, leading to organ-protective effects. DHP-CCBs have a potent blood pressure–lowering effect and suppress atherosclerosis and coronary vasospasm. Diltiazem, a non-DHP-CCB, is highly effective for vasospasm control. CCBs reduce left ventricular hypertrophy and arterial stiffness. Amlodipine, a DHP-CCB, reduces blood pressure variability. L/N- and L/T-type CCBs combined with renin-angiotensin system blockers reduce proteinuria and improve kidney function compared with L-type CCBs. According to large-scale trials, DHP-CCBs reduce cardiovascular events in patients with isolated systolic hypertension, as well as in elderly and high-risk patients. Accordingly, CCBs are indicated for hypertension in elderly patients, isolated systolic hypertension, angina pectoris, and coronary vasospasm. Non-DHP-CCBs are contraindicated in high-grade heart block, bradycardia (<60 beats per minute [bpm]), and heart failure with reduced ejection fraction (HFrEF). DHP-CCBs should be used with caution in patients with tachyarrhythmia, HFrEF, and severe leg edema, and non-DHP-CCBs should be used carefully in those with constipation. Each CCB has distinct pharmacokinetics and side effects, underscoring the need for meticulous consideration in clinical practice.
Figure
-
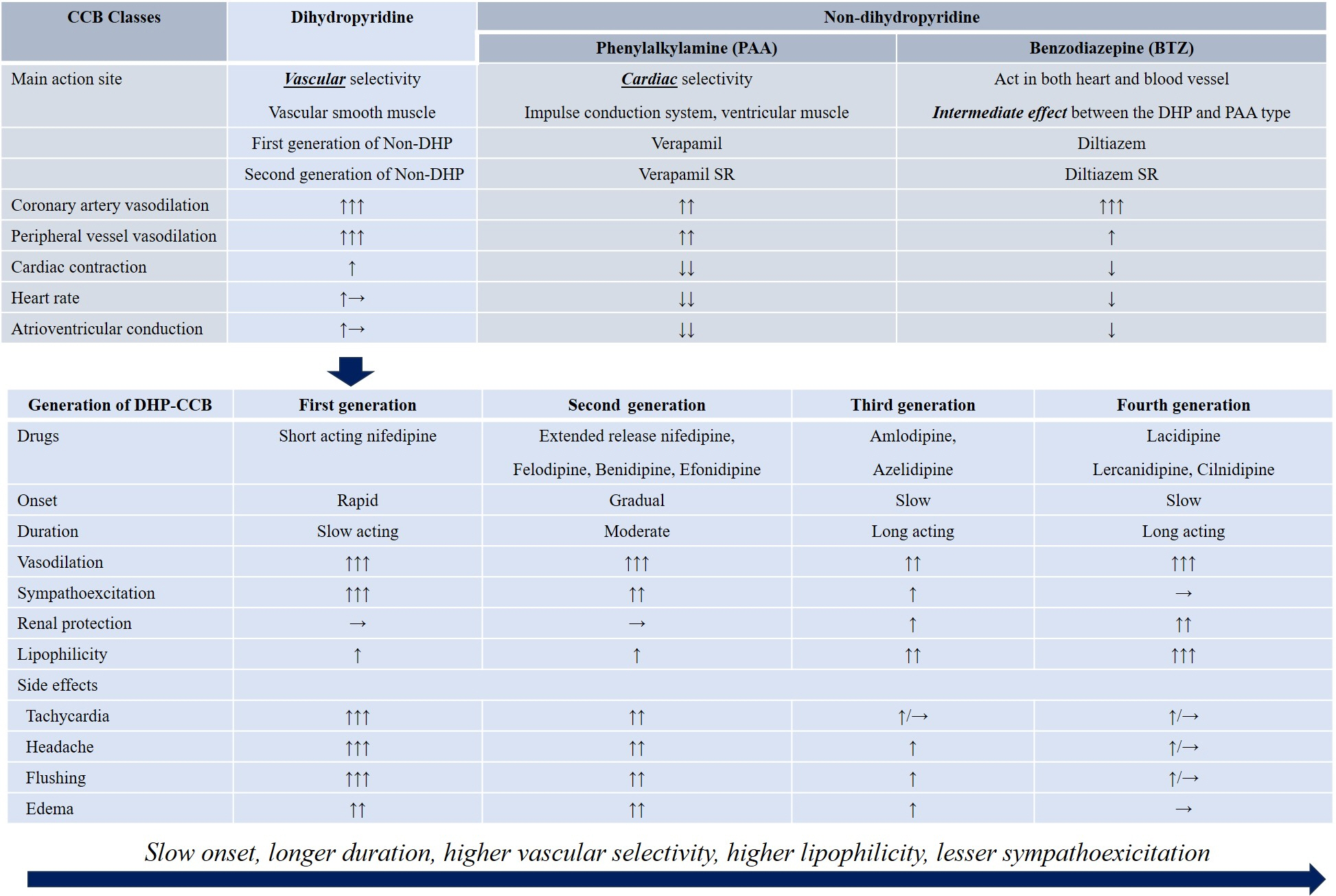
Fig. 1. Classification and pharmacological actions of calcium channel blockers (CCBs). DHP, dihydropyridine; PAA, benzodiazepine; Non-DHP, non-dihydropyridine; SR, sustained release; ↑↑↑, strongest; ↑↑, very strong; ↑, strong positive action; →, neutral action; ↓, negative action.Based on data from Sueta et al. [3], and Wang et al. [4], Elliott et al. [5], Wang et al. [6].
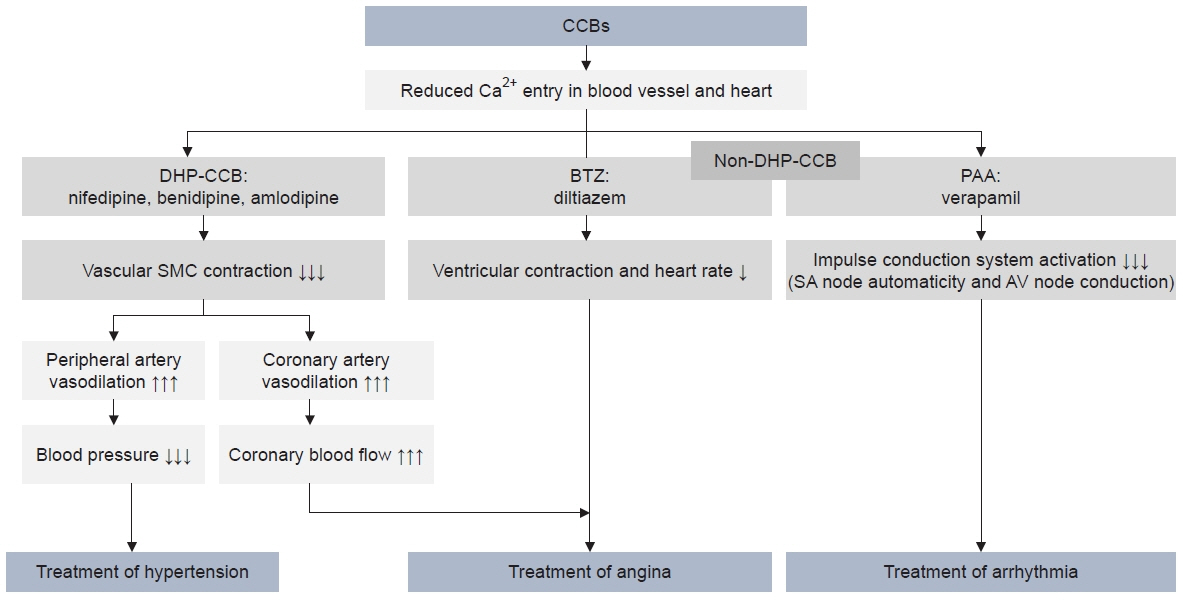
Fig. 2. Three main pharmacological mechanisms of calcium channel blockers (CCBs): treatment of hypertension through peripheral vasodilation; treatment of angina pectoris through coronary artery vasodilation and decreased ventricular contraction and heart rate; and arrhythmia treatment through decreased impulse conduction system excitation. Downward arrow indicate negative action, upward arrow indicate positive action (the degree is presented by the number of arrows). DHP, dihydropyridine; BTZ, benzothiazepine; PAA, phenylalkylamine; SMC, smooth muscle cell; SA node, sinoatrial node; AV node, atrioventricular node.Based on data from Sueta et al. [3].

Fig. 3. Voltage-gated calcium channels and three representative types. (A) Voltage-gated calcium channels. Voltage-gated extracellular calcium (Ca2+) channels consist of four subunits, α1 and α2, δ, β, and γ, and they are pharmacologically classified into different subtypes; the characteristics of which are determined by the pore-forming α1 subunit. Calcium channel blockers (CCBs) disrupt the inward movement of Ca2+ through the calcium channel. (B) Three representative types of calcium channel. Calcium channels are pharmacologically classified into different subtypes: high voltage–activated (L- and N-type) and low voltage–activated (T-type). L-type channels act as potent vasodilators, N-type channels have decreased norepinephrine (NE) release in the sympathetic nerve ending, and T-type channels have improvement of renal microcirculation. It is speculated that the combined blocking of N- or T-channels in addition to traditional L-type blocking in CCBs leads to different pharmacologic impacts and adverse effects of dihydropyridine CCBs.
Reference
-
1. Kim HC, Lee H, Lee HH, Lee G, Kim E, Song M, et al. Korea hypertension fact sheet 2022: analysis of nationwide population-based data with a special focus on hypertension in the elderly. Clin Hypertens. 2023; 29:22.2. Kim HL, Lee EM, Ahn SY, Kim KI, Kim HC, Kim JH, et al. The 2022 focused update of the 2018 Korean Hypertension Society Guidelines for the management of hypertension. Clin Hypertens. 2023; 29:11.3. Sueta D, Tabata N, Hokimoto S. Clinical roles of calcium channel blockers in ischemic heart diseases. Hypertens Res. 2017; 40:423–8.4. Wang AL, Iadecola C, Wang G. New generations of dihydropyridines for treatment of hypertension. J Geriatr Cardiol. 2017; 14:67–72.5. Elliott WJ, Ram CV. Calcium channel blockers. J Clin Hypertens (Greenwich). 2011; 13:687–9.6. Wang JG, Kario K, Lau T, Wei YQ, Park CG, Kim CH, et al. Use of dihydropyridine calcium channel blockers in the management of hypertension in Eastern Asians: a scientific statement from the Asian Pacific Heart Association. Hypertens Res. 2011; 34:423–30.7. Chandra KS, Ramesh G. The fourth-generation Calcium channel blocker: cilnidipine. Indian Heart J. 2013; 65:691–5.8. Mancia G, Kreutz R, Brunstrom M, Burnier M, Grassi G, Januszewicz A, et al. 2023 ESH Guidelines for the management of arterial hypertension The Task Force for the management of arterial hypertension of the European Society of Hypertension endorsed by the International Society of Hypertension (ISH) and the European Renal Association (ERA). J Hypertens 2023 Jun 21 [Epub]. https://doi.org/10.1097/HJH.0000000000003480.9. Robles NR, Fici F, Grassi G. Dihydropyridine calcium channel blockers and renal disease. Hypertens Res. 2017; 40:21–8.10. Furukawa T, Yamakawa T, Midera T, Sagawa T, Mori Y, Nukada T. Selectivities of dihydropyridine derivatives in blocking Ca(2+) channel subtypes expressed in Xenopus oocytes. J Pharmacol Exp Ther. 1999; 291:464–73.11. Ge W, Ren J. Combined L-/T-type calcium channel blockers: ready for prime time. Hypertension. 2009; 53:592–4.12. Hayashi K. L-/T-type Ca channel blockers for kidney protection: ready for sophisticated use of Ca channel blockers. Hypertens Res. 2011; 34:910–2.13. Yao K, Nagashima K, Miki H. Pharmacological, pharmacokinetic, and clinical properties of benidipine hydrochloride, a novel, long-acting calcium channel blocker. J Pharmacol Sci. 2006; 100:243–61.14. Ram CV. Therapeutic usefulness of a novel calcium channel blocker azelnidipine in the treatment of hypertension: a narrative review. Cardiol Ther. 2022; 11:473–89.15. Packer M, Carson P, Elkayam U, Konstam MA, Moe G, O’Connor C, et al. Effect of amlodipine on the survival of patients with severe chronic heart failure due to a nonischemic cardiomyopathy: results of the PRAISE-2 study (Prospective Randomized Amlodipine Survival Evaluation 2). JACC Heart Fail. 2013; 1:308–14.16. Thamcharoen N, Susantitaphong P, Wongrakpanich S, Chongsathidkiet P, Tantrachoti P, Pitukweerakul S, et al. Effect of N- and T-type calcium channel blocker on proteinuria, blood pressure and kidney function in hypertensive patients: a meta-analysis. Hypertens Res. 2015; 38:847–55.17. Ferri N, Corsini A, Pontremoli R. Antihypertensive treatment with calcium channel blockers and renal protection: focus on lercanidipine and lercanidipine/enalapril. Eur Rev Med Pharmacol Sci. 2022; 26:7482–92.18. Fleckenstein A, Tritthart H, Flackenstein B, Herbst A, Grun G. A new group of competitive divalent Ca-antagonists (iproveratril, D 600, prenylamine) with potent inhibitory effects on electromechanical coupling in mammalian myocardium. Pflugers Arch. 1969; 307:R25.19. Ozawa Y, Hayashi K, Kobori H. New generation calcium channel blockers in hypertensive treatment. Curr Hypertens Rev. 2006; 2:103–11.20. Yousef WM, Omar AH, Morsy MD, Abd El-Wahed MM, Ghanayem NM. The mechanism of action of calcium channel blockers in the treatment of diabetic nephropathy. Dubai Diabetes Endocrinol J. 2005; 13:76–82.21. Hayashi K, Wakino S, Sugano N, Ozawa Y, Homma K, Saruta T. Ca2+ channel subtypes and pharmacology in the kidney. Circ Res. 2007; 100:342–53.22. Ghamami N, Chiang SH, Dormuth C, Wright JM. Time course for blood pressure lowering of dihydropyridine calcium channel blockers. Cochrane Database Syst Rev. 2014; (8):CD010052.23. Lorimer AR, Lyons D, Fowler G, Petrie JC, Rothman MT. Differences between amlodipine and lisinopril in control of clinic and twenty-four hour ambulatory blood pressures. J Hum Hypertens. 1998; 12:411–6.24. Rothwell PM, Howard SC, Dolan E, O’Brien E, Dobson JE, Dahlof B, et al. Prognostic significance of visit-to-visit variability, maximum systolic blood pressure, and episodic hypertension. Lancet. 2010; 375:895–905.25. Dahlof B, Sever PS, Poulter NR, Wedel H, Beevers DG, Caulfield M, et al. Prevention of cardiovascular events with an antihypertensive regimen of amlodipine adding perindopril as required versus atenolol adding bendroflumethiazide as required, in the Anglo-Scandinavian Cardiac Outcomes Trial-Blood Pressure Lowering Arm (ASCOT-BPLA): a multicentre randomised controlled trial. Lancet. 2005; 366:895–906.26. Webb AJ, Fischer U, Mehta Z, Rothwell PM. Effects of antihypertensive-drug class on interindividual variation in blood pressure and risk of stroke: a systematic review and meta-analysis. Lancet. 2010; 375:906–15.27. Muntner P, Levitan EB, Lynch AI, Simpson LM, Whittle J, Davis BR, et al. Effect of chlorthalidone, amlodipine, and lisinopril on visit-to-visit variability of blood pressure: results from the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial. J Clin Hypertens (Greenwich). 2014; 16:323–30.28. Schmieder RE, Martus P, Klingbeil A. Reversal of left ventricular hypertrophy in essential hypertension: a meta-analysis of randomized double-blind studies. JAMA. 1996; 275:1507–13.29. Klingbeil AU, Schneider M, Martus P, Messerli FH, Schmieder RE. A meta-analysis of the effects of treatment on left ventricular mass in essential hypertension. Am J Med. 2003; 115:41–6.30. Koracevic G, Perisic Z, Stanojkovic M, Stojanovic M, Zdravkovic M, Tomasevic M, et al. A discrepancy: calcium channel blockers are effective for the treatment of hypertensive left ventricular hypertrophy but not as effective for prevention of heart failure. Med Princ Pract. 2022; 31:454–62.31. ALLHAT Officers and Coordinators for the ALLHAT Collaborative Research Group. Major outcomes in moderately hypercholesterolemic, hypertensive patients randomized to pravastatin vs usual care: the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT-LLT). JAMA. 2002; 288:2998–3007.32. Boutouyrie P, Chowienczyk P, Humphrey JD, Mitchell GF. Arterial stiffness and cardiovascular risk in hypertension. Circ Res. 2021; 128:864–86.33. Hayoz D, Zappe DH, Meyer MA, Baek I, Kandra A, Joly MP, et al. Changes in aortic pulse wave velocity in hypertensive postmenopausal women: comparison between a calcium channel blocker vs angiotensin receptor blocker regimen. J Clin Hypertens (Greenwich). 2012; 14:773–8.34. Takami T, Shigemasa M. Efficacy of various antihypertensive agents as evaluated by indices of vascular stiffness in elderly hypertensive patients. Hypertens Res. 2003; 26:609–14.35. Matsui Y, Eguchi K, O’Rourke MF, Ishikawa J, Miyashita H, Shimada K, et al. Differential effects between a calcium channel blocker and a diuretic when used in combination with angiotensin II receptor blocker on central aortic pressure in hypertensive patients. Hypertension. 2009; 54:716–23.36. Henry PD, Bentley KI. Suppression of atherogenesis in cholesterol-fed rabbit treated with nifedipine. J Clin Invest. 1981; 68:1366–9.37. Pitt B, Byington RP, Furberg CD, Hunninghake DB, Mancini GB, Miller ME, et al. Effect of amlodipine on the progression of atherosclerosis and the occurrence of clinical events. Circulation. 2000; 102:1503–10.38. Zanchetti A, Bond MG, Hennig M, Neiss A, Mancia G, Dal Palu C, et al. Calcium antagonist lacidipine slows down progression of asymptomatic carotid atherosclerosis: principal results of the European Lacidipine Study on Atherosclerosis (ELSA), a randomized, double-blind, long-term trial. Circulation. 2002; 106:2422–7.39. Ishii N, Matsumura T, Shimoda S, Araki E. Anti-atherosclerotic potential of dihydropyridine calcium channel blockers. J Atheroscler Thromb. 2012; 19:693–704.40. Nishigaki K, Inoue Y, Yamanouchi Y, Fukumoto Y, Yasuda S, Sueda S, et al. Prognostic effects of calcium channel blockers in patients with vasospastic angina: a meta-analysis. Circ J. 2010; 74:1943–50.41. Kim SE, Jo SH, Han SH, Lee KY, Her SH, Lee MH, et al. Comparison of calcium-channel blockers for long-term clinical outcomes in patients with vasospastic angina. Korean J Intern Med. 2021; 36:124–34.42. Jamerson K, Weber MA, Bakris GL, Dahlof B, Pitt B, Shi V, et al. Benazepril plus amlodipine or hydrochlorothiazide for hypertension in high-risk patients. N Engl J Med. 2008; 359:2417–28.43. Bakris GL, Sarafidis PA, Weir MR, Dahlof B, Pitt B, Jamerson K, et al. Renal outcomes with different fixed-dose combination therapies in patients with hypertension at high risk for cardiovascular events (ACCOMPLISH): a prespecified secondary analysis of a randomised controlled trial. Lancet. 2010; 375:1173–81.44. Abe M, Soma M. Multifunctional L/N- and L/T-type calcium channel blockers for kidney protection. Hypertens Res. 2015; 38:804–6.45. Burnier M. Renal protection with calcium antagonists: the role of lercanidipine. Curr Med Res Opin. 2013; 29:1727–35.46. Zhao M, Zhang Z, Pan Z, Ma S, Chang M, Fan J, et al. N-/T-type vs. L-type calcium channel blocker in treating chronic kidney disease: a systematic review and meta-analysis. Pharmaceuticals (Basel). 2023; 16:338.47. Staessen JA, Fagard R, Thijs L, Celis H, Arabidze GG, Birkenhager WH, et al. Randomised double-blind comparison of placebo and active treatment for older patients with isolated systolic hypertension. The Systolic Hypertension in Europe (Syst-Eur) Trial Investigators. Lancet. 1997; 350:757–64.48. Brown MJ, Palmer CR, Castaigne A, de Leeuw PW, Mancia G, Rosenthal T, et al. Morbidity and mortality in patients randomised to double-blind treatment with a long-acting calcium-channel blocker or diuretic in the International Nifedipine GITS study: Intervention as a Goal in Hypertension Treatment (INSIGHT). Lancet. 2000; 356:366–72.49. Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL Jr, et al. The seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA. 2003; 289:2560–72.50. Julius S, Kjeldsen SE, Weber M, Brunner HR, Ekman S, Hansson L, et al. Outcomes in hypertensive patients at high cardiovascular risk treated with regimens based on valsartan or amlodipine: the VALUE randomised trial. Lancet. 2004; 363:2022–31.51. Gupta A, Mackay J, Whitehouse A, Godec T, Collier T, Pocock S, et al. Long-term mortality after blood pressure-lowering and lipid-lowering treatment in patients with hypertension in the Anglo-Scandinavian Cardiac Outcomes Trial (ASCOT) Legacy study: 16-year follow-up results of a randomised factorial trial. Lancet. 2018; 392:1127–37.52. Sica D. Calcium channel blocker-related periperal edema: can it be resolved? J Clin Hypertens (Greenwich). 2003; 5:291–4. 29753. Liang L, Kung JY, Mitchelmore B, Cave A, Banh HL. Comparative peripheral edema for dihydropyridines calcium channel blockers treatment: a systematic review and network meta-analysis. J Clin Hypertens (Greenwich). 2022; 24:536–54.54. Zanchetti A. Emerging data on calcium-channel blockers: the COHORT study. Clin Cardiol. 2003; 26(2 Suppl 2):II17–20.55. Makani H, Bangalore S, Romero J, Htyte N, Berrios RS, Makwana H, et al. Peripheral edema associated with calcium channel blockers: incidence and withdrawal rate: a meta-analysis of randomized trials. J Hypertens. 2011; 29:1270–80.56. Vouri SM, Jiang X, Manini TM, Solberg LM, Pepine C, Malone DC, et al. Magnitude of and characteristics associated with the treatment of calcium channel blocker-induced lower-extremity edema with loop diuretics. JAMA Netw Open. 2019; 2:e1918425.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A case of gingival hyperplasia caused by amlodipine
- A case of gingival hyperplasia caused by felodipine
- Effects of Calcium Channel Blockers on Cardiopulmonary Hemodynamics in Dogs
- The Effect of Oral Calcium Channel Blockers on the Ocular Blood Flow
- Chlorthalidone, not hydrochlorothiazide, is the right diuretic for comparison
