Spontaneous hepatic arterioportal fistula in extrahepatic portal vein obstruction: Combined endovascular and surgical management
- Affiliations
-
- 1Department of Diagnostic and Interventional Radiology, All India Institute of Medical Sciences, Jodhpur, Rajasthan, India
- 2Department of Gastrointestinal Surgery, All India Institute of Medical Sciences, Jodhpur, Rajasthan, India
- KMID: 2545778
- DOI: http://doi.org/10.14701/ahbps.22-126
Abstract
- Hepatic arterioportal fistulae are abnormal communications between the hepatic artery and portal vein. They are reported to be congenital or acquired secondary to trauma, iatrogenic procedures, hepatic cirrhosis, and hepatocellular carcinoma, but less likely to occur spontaneously. Extrahepatic portal venous obstruction (EHPVO) can lead to pre-hepatic portal hypertension. A spontaneous superimposed hepatic arterioportal fistula can lead to pre-sinusoidal portal hypertension, further exacerbating its physiology. This report describes a young woman with long-standing EHPVO presenting with repeated upper gastrointestinal variceal bleeding and symptomatic hypersplenism. Computed tomography scan demonstrated a cavernous transformation of the portal vein and a macroscopic hepatic arterioportal fistula between the left hepatic artery and portal vein collateral in the central liver. The hepatic arterioportal fistula was associated with a flow-related left hepatic artery aneurysm and a portal venous collateral aneurysm proximal and distal to the fistula, respectively. Endovascular coiling was performed for the hepatic arterioportal fistula, followed by proximal splenorenal shunt procedure. This case illustrates an uncommon association of a spontaneous hepatic arterioportal fistula with EHPVO and the utility of a combined endovascular and surgical approach for managing multifactorial non-cirrhotic portal hypertension in such patients.
Keyword
Figure
-
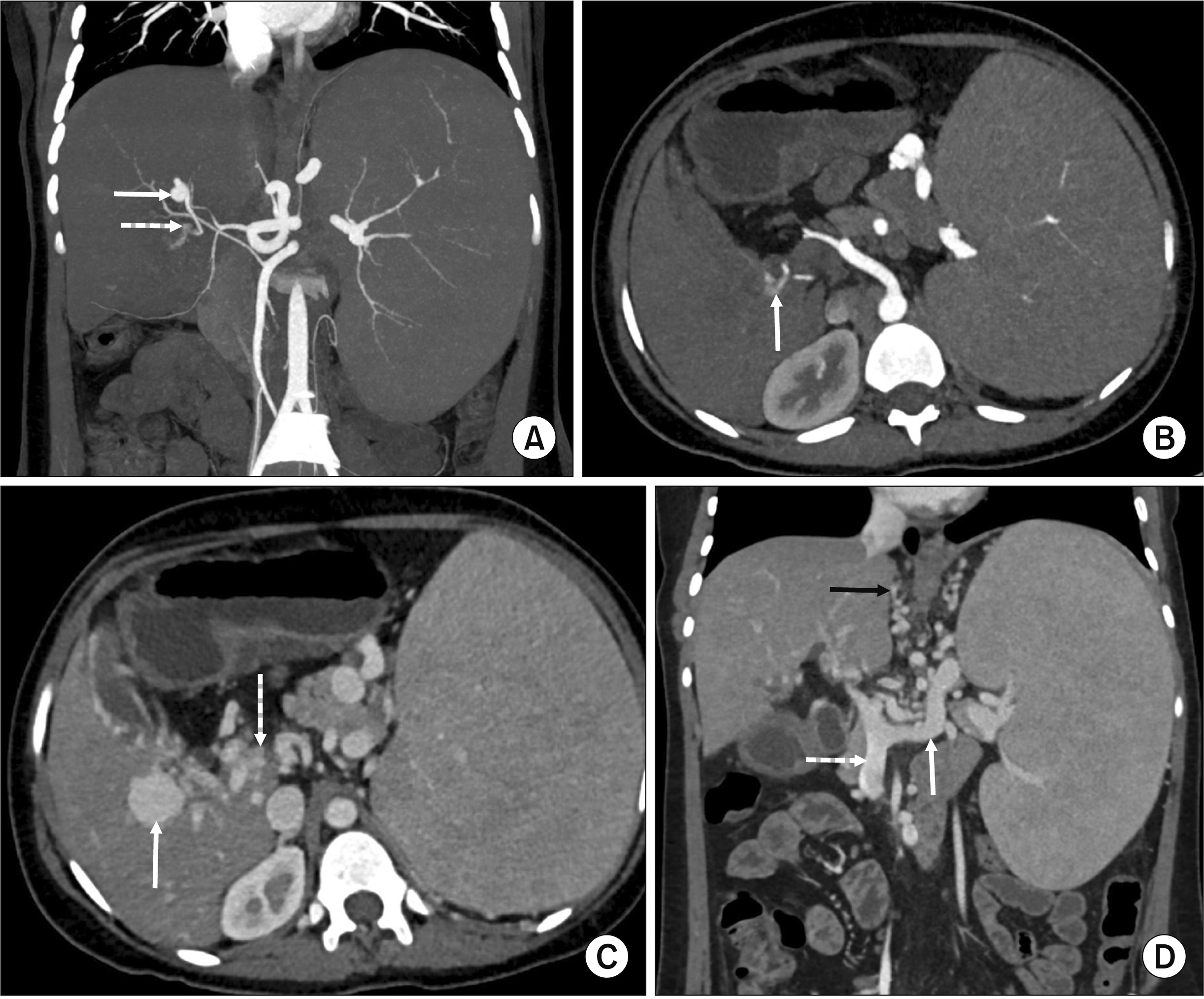
Fig. 1 (A) Coronal maximum intensity projection image from arterial phase computed tomography (CT) demonstrating a left hepatic artery aneurysm (solid white arrow) with a large branch leading to early arterial opacification of portal venous collateral (dashed white arrow) suggestive of hepatic arterioportal fistula (HAPF). (B) Axial thin section arterial phase CT at the level of portal venous collateral demonstrating early arterial opacification of portal venous collateral (arrow) before opacification of splenic and superior mesenteric veins consistent with HAPF. (C) Axial thin section venous phase CT at the level of portal venous collateral (same as B) demonstrating a portal collateral vein aneurysm (solid white arrow) distal to the HAPF. Also shown is a cavernous transformation of extrahepatic portal vein (dashed white arrow) consistent with extrahepatic portal venous obstruction (EHPVO). (D) Coronal multiplanar reformat image from venous phase CT demonstrating additional findings of EHPVO such as portosystemic collaterals (black arrow) and massive splenomegaly. The superior mesenteric vein (dashed white arrow) and splenic vein (solid white arrow) were patent in this case.

Fig. 2 Volume rendered technique image from arterial phase computed tomography demonstrating the spectrum of arterial findings, including left hepatic artery (LHA) aneurysm and macroscopic hepatic arterioportal fistula (HAPF) with arterial opacification of portal vein collateral. Also note the replaced right hepatic artery (RHA) arising from superior mesenteric artery (SMA) coursing posterior to the HAPF and the markedly ectatic splenic artery with small aneurysm.

Fig. 3 Selected digital subtraction angiogram images demonstrating endovascular management of hepatic arterioportal fistula (HAPF). Pre-embolization images from common hepatic artery angiogram (A) and left hepatic artery angiogram (B) demonstrating the left hepatic artery aneurysm (solid black arrow in A), shunting of arterial blood into a portal venous channel (dashed black arrows in A, B), and the macroscopic fistulous connection between left hepatic artery and the portal venous collateral (solid black arrow in B). (C) Post- embolization image from left hepatic artery angiogram showing complete obliteration of both left hepatic artery aneurysm and HAPF with no residual flow.

Fig. 4 (A) Coronal maximum intensity projection image from portal venous phase computed tomography (CT) demonstrating endovascular coil in left hepatic artery (solid black arrow). The splenorenal shunt is patent (black arrow with white outline). Proximal splenic vein (solid white arrow) and left renal vein (dashed white arrow) draining into the inferior vena cava are expected to be prominent. The replaced right hepatic artery is denoted by a dashed black arrow. Axial (B) and coronal (C) thin section portal venous phase CT at the level of porta demonstrating resolution of portal cavernoma without any residual portal vein collateral aneurysm (white arrows). The peribiliary venous plexus has also regressed with resolved central intrahepatic biliary dilation. (D) Coronal multiplanar reformat image from venous phase CT demonstrating expected changes of proximal splenorenal shunt with splenectomy, resolution of portosystemic collaterals and dilation of splenic vein (solid white arrow), and superior mesenteric vein (dashed white arrow) due to diversion of portal circulation.
Reference
-
1. Sarin SK, Kumar A. 2006; Noncirrhotic portal hypertension. Clin Liver Dis. 10:627–651. DOI: 10.1016/j.cld.2006.08.021. PMID: 17162232.2. Poddar U, Thapa BR, Rao KL, Singh K. 2008; Etiological spectrum of esophageal varices due to portal hypertension in Indian children: is it different from the West? J Gastroenterol Hepatol. 23:1354–1357. DOI: 10.1111/j.1440-1746.2007.05102.x. PMID: 17683492.3. Sarin SK, Agarwal SR. 2002; Extrahepatic portal vein obstruction. Semin Liver Dis. 22:43–58. DOI: 10.1055/s-2002-23206. PMID: 11928078.4. Sarin SK, Sollano JD, Chawla YK, Amarapurkar D, Hamid S, Hashizume M, et al. 2006; Consensus on extra-hepatic portal vein obstruction. Liver Int. 26:512–519. DOI: 10.1111/j.1478-3231.2006.01269.x. PMID: 16761994.5. Guzman EA, McCahill LE, Rogers FB. 2006; Arterioportal fistulas: introduction of a novel classification with therapeutic implications. J Gastrointest Surg. 10:543–550. DOI: 10.1016/j.gassur.2005.06.022. PMID: 16627220.6. Cao B, Tian K, Zhou H, Li C, Liu D, Tan Y. 2022; Hepatic arterioportal fistulas: a retrospective analysis of 97 cases. J Clin Transl Hepatol. 10:620–626. DOI: 10.14218/JCTH.2021.00100. PMID: 36062281. PMCID: PMC9396316.7. Sarin SK, Lahoti D, Saxena SP, Murthy NS, Makwana UK. 1992; Prevalence, classification and natural history of gastric varices: a long-term follow-up study in 568 portal hypertension patients. Hepatology. 16:1343–1349. DOI: 10.1002/hep.1840160607. PMID: 1446890.8. Khanna R, Sarin SK. 2014; Non-cirrhotic portal hypertension - diagnosis and management. J Hepatol. 60:421–441. DOI: 10.1016/j.jhep.2013.08.013. PMID: 23978714.9. Rajesh S, Mukund A, Sureka B, Bansal K, Ronot M, Arora A. 2018; Non-cirrhotic portal hypertension: an imaging review. Abdom Radiol (NY). 43:1991–2010. DOI: 10.1007/s00261-018-1570-8. PMID: 29564495.10. Vauthey JN, Tomczak RJ, Helmberger T, Gertsch P, Forsmark C, Caridi J, et al. 1997; The arterioportal fistula syndrome: clinicopathologic features, diagnosis, and therapy. Gastroenterology. 113:1390–1401. DOI: 10.1053/gast.1997.v113.pm9322535. PMID: 9322535.11. Choi BI, Chung JW, Itai Y, Matsui O, Han JK, Han MC. 1999; Hepatic abnormalities related to blood flow: evaluation with dual-phase helical CT. Abdom Imaging. 24:340–356. DOI: 10.1007/s002619900512. PMID: 10390555.12. Wang Q, Koniaris LG, Milgrom DP, Patel A, Hu M, Cui E, et al. 2019; CT and MRI imaging and interpretation of hepatic arterioportal shunts. Transl Gastroenterol Hepatol. 4:34. DOI: 10.21037/tgh.2019.05.05. PMID: 31231701. PMCID: PMC6556701.13. Itai Y, Moss AA, Goldberg HI. 1982; Transient hepatic attenuation difference of lobar or segmental distribution detected by dynamic computed tomography. Radiology. 144:835–839. DOI: 10.1148/radiology.144.4.6287520. PMID: 6287520.14. Liu GF, Wang XZ, Luo XF. 2021; Simultaneous embolization of a spontaneous porto-systemic shunt and intrahepatic arterioportal fistula: a case report. World J Clin Cases. 9:9577–9583. DOI: 10.12998/wjcc.v9.i31.9577. PMID: 34877293. PMCID: PMC8610867.15. Hirakawa M, Nishie A, Asayama Y, Ishigami K, Ushijima Y, Fujita N, et al. 2013; Clinical outcomes of symptomatic arterioportal fistulas after transcatheter arterial embolization. World J Radiol. 5:33–40. DOI: 10.4329/wjr.v5.i2.33. PMID: 23494252. PMCID: PMC3596609.16. Chaudry G, Lillis AP, Shaikh R, Padua HM, Chewning RH, Alomari AI. 2018; Endovascular treatment of congenital arterioportal fistulas. Cardiovasc Intervent Radiol. 41:1021–1028. DOI: 10.1007/s00270-018-1924-1. PMID: 29511867.17. Lal R, Sarma MS, Gupta MK. 2017; Extrahepatic portal venous obstruction: what should be the mainstay of treatment? Indian J Pediatr. 84:691–699. DOI: 10.1007/s12098-017-2390-5. PMID: 28612224.18. Poddar U, Borkar V. 2011; Management of extra hepatic portal venous obstruction (EHPVO): current strategies. Trop Gastroenterol. 32:94–102. PMID: 21922871.19. Rajalingam R, Javed A, Sharma D, Sakhuja P, Singh S, Nag HH, et al. 2012; Management of hypersplenism in non-cirrhotic portal hypertension: a surgical series. Hepatobiliary Pancreat Dis Int. 11:165–171. DOI: 10.1016/S1499-3872(12)60143-X. PMID: 22484585.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Endovascular treatment of psuedoaneurysm arising from common hepatic artery bifurcation with complete disruption of gastroduodenal artery and high flow arterioportal fistula
- Gastroesophageal Bleeding Due to Intrahepatic Arterioportal Fistula: A Case Report of Treatment with Occlusive Balloon and Coils
- A Case of Hepatic Artery-Portal Vein Fistula
- Use of meso-Rex shunt with transposition of the coronary vein for the management of extrahepatic portal vein obstruction
- Hepatic Arterioportal Shunts: Dynamic CT and MR Features
