First Experience of Single-Port Robotic Areolar Approach Thyroidectomy
- Affiliations
-
- 1Department of Surgery, Inha University Hospital, Inha University College of Medicine, Incheon, Korea
- 2Robot Surgery Center, Inha University Hospital, Inha University College of Medicine, Incheon, Korea
- KMID: 2545266
- DOI: http://doi.org/10.21053/ceo.2023.00682
Abstract
Objectives
. Numerous minimally invasive thyroidectomy techniques have been developed and are actively utilized in hospitals around the globe. Herein, we describe a recently developed minimally invasive thyroidectomy technique that employs the da Vinci SP, and we present the preliminary clinical outcomes of single-port robotic areolar thyroidectomy (SPRA).
Methods
. A 3-cm semi-circular incision on the right areola and a small 8-mm incision on the left areola were created. Using hydro-dissection and an advanced bipolar device, a subcutaneous skin flap was created, extending from the areola to the thyroid cartilage. The da Vinci SP was then inserted through the incision in the right areola. Between December 2022 and March 2023, 21 SPRA procedures were conducted. Patients’ medical records and surgical videos were subsequently reviewed.
Results
. Lobectomy was performed in 17 patients, isthmectomy in 2 patients, and total thyroidectomy in 2 patients. The mean flap time was 14.9±4.2 minutes and the console time was 62.4±17.1 minutes. The mean tumor size was 0.89± 0.65 cm and the number of retrieved lymph nodes was 3.94±3.98 (range, 0–12). There were no observed instances of vocal cord palsy or hypoparathyroidism.
Conclusion
. We successfully developed and performed the novel SPRA for the first time worldwide. Unlike other robotic surgery methods, SPRA is less invasive and leaves no visible scars. This technique employs a sophisticated single-port robotic device. However, to assess the efficacy of this method, we need to analyze more cases and conduct comparative studies in the near future.
Figure
-
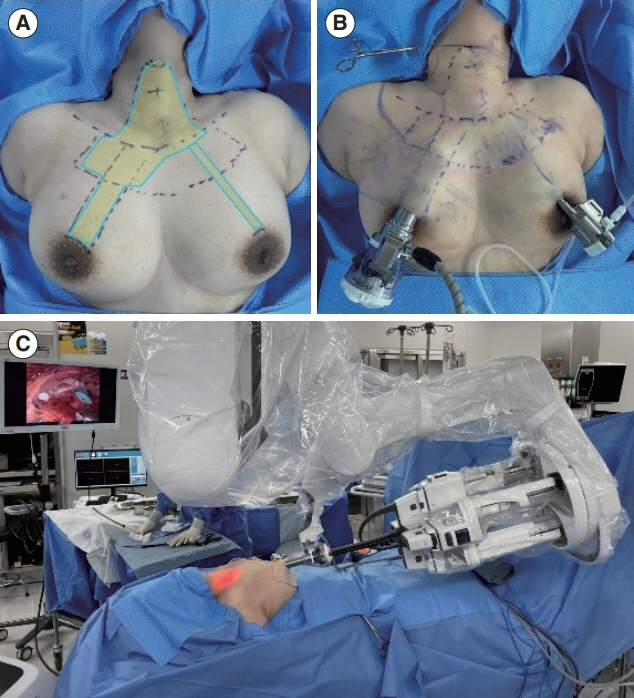
Fig. 1. Creation of the flap for single-port robotic areolar thyroidectomy (SPRA) and docking of the da Vinci SP. (A) The process of creating the flap for SPRA. (B) The status of port insertion for SPRA. (C) The docking status of the da Vinci SP for SPRA.
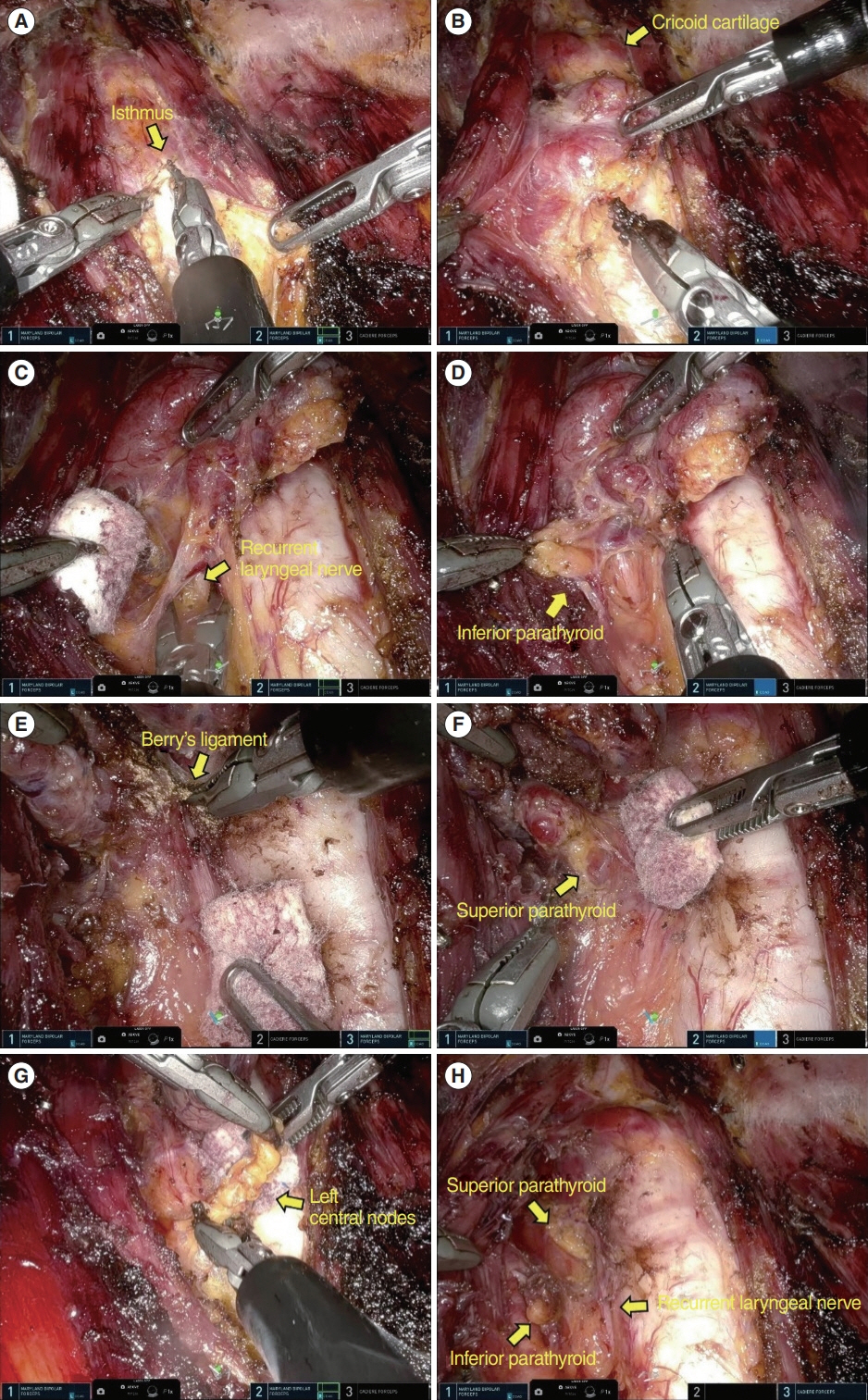
Fig. 2. Procedure for the single-port robotic areolar thyroidectomy operation. (A) The strap muscle's midline and the thyroid isthmus were divided. (B) The thyroid gland was moved to the opposite side, and the area between the thyroid gland and strap muscle was dissected. (C) The thyroid gland was then elevated, and the recurrent laryngeal nerve was identified. (D) The inferior parathyroid gland was preserved, and the thyroid gland was detached from the trachea. (E) The thyroid gland was shifted to the superior pole, and Berry’s ligament was dissected. (F) The superior parathyroid gland was identified and preserved, and a thyroidectomy was performed after the superior thyroid vessels were coagulated. (G) A level 6 central lymph node dissection was performed between the carotid artery and trachea, without impacting the recurrent laryngeal nerve. (H) Both the recurrent laryngeal nerve and the two parathyroid glands were successfully preserved.

Fig. 3. Postoperative wound after single-port robotic areolar thyroidectomy
Reference
-
1. Davies L, Welch HG. Current thyroid cancer trends in the United States. JAMA Otolaryngol Head Neck Surg. 2014; Apr. 140(4):317–22.2. Zhai M, Zhang D, Long J, Gong Y, Ye F, Liu S, et al. The global burden of thyroid cancer and its attributable risk factor in 195 countries and territories: a systematic analysis for the Global Burden of Disease Study. Cancer Med. 2021; Jul. 10(13):4542–54.3. Health Insurance Review and Assessment Service (HIRA). HIRA bigdata open portal [Internet]. HIRA;2022. [cited 2023 Jul 25]. Available from: https://opendata.hira.or.kr/home.do.4. Randolph GW. Surgery of the thyroid and parathyroid glands. 3rd ed. 2013. Elsevier.5. Arora A, Swords C, Garas G, Chaidas K, Prichard A, Budge J, et al. The perception of scar cosmesis following thyroid and parathyroid surgery: a prospective cohort study. Int J Surg. 2016; Jan. 25:38–43.6. de Vries LH, Aykan D, Lodewijk L, Damen JA, Borel Rinkes IH, Vriens MR. Outcomes of minimally invasive thyroid surgery: a systematic review and meta-analysis. Front Endocrinol (Lausanne). 2021; Aug. 12:719397.7. Tae K, Ji YB, Song CM, Ryu J. Robotic and endoscopic thyroid surgery: evolution and advances. Clin Exp Otorhinolaryngol. 2019; Feb. 12(1):1–11.8. Ruhle BC, Ferguson Bryan A, Grogan RH. Robot-assisted endocrine surgery: indications and drawbacks. J Laparoendosc Adv Surg Tech A. 2019; Feb. 29(2):129–35.9. Choe JH, Kim SW, Chung KW, Park KS, Han W, Noh DY, et al. Endoscopic thyroidectomy using a new bilateral axillo-breast approach. World J Surg. 2007; Mar. 31(3):601–6.10. Lee KE, Rao J, Youn YK. Endoscopic thyroidectomy with the da Vinci robot system using the bilateral axillary breast approach (BABA) technique: our initial experience. Surg Laparosc Endosc Percutan Tech. 2009; Jun. 19(3):e71–5.11. Kwak J, Yu HW, Lee KE. Bilateral axillo-breast approach robotic thyroid surgery. Ann Robot Innov Surg. 2020; Dec. 1(2):69–80.12. Ryu HB, Ahn JH, Kim JH, Choi SW, Choi YS, Yi JW. Harmonic versus LigaSure for flap creation in bilateral axillary breast approach thyroid surgery. J Endocr Surg. 2020; Dec. 20(4):69–77.13. Choi YS, Shin WY, Yi JW. Single surgeon experience with 500 cases of the robotic bilateral axillary breast approach (BABA) for thyroid surgery using the Da-Vinci Xi system. J Clin Med. 2021; Sep. 10(18):4048.14. Vaccarella S, Franceschi S, Bray F, Wild CP, Plummer M, Dal Maso L. Worldwide thyroid-cancer epidemic?: the increasing impact of overdiagnosis. N Engl J Med. 2016; Aug. 375(7):614–7.15. Dordea M, Aspinall SR. Short and long-term cosmesis of cervical thyroidectomy scars. Ann R Coll Surg Engl. 2016; Jan. 98(1):11–7.16. Qiu TY, Lau J, Wong O, Oh HB, Boon TW, Parameswaran R, et al. Preoperative scar perception study comparing ‘scarless’ in the neck endoscopic thyroidectomy with open thyroidectomy: a cross-sectional study. Ann R Coll Surg Engl. 2020; Nov. 102(9):737–43.17. Kang SW, Jeong JJ, Yun JS, Sung TY, Lee SC, Lee YS, et al. Robot-assisted endoscopic surgery for thyroid cancer: experience with the first 100 patients. Surg Endosc. 2009; Nov. 23(11):2399–406.18. Kim MJ, Nam KH, Lee SG, Choi JB, Kim TH, Lee CR, et al. Yonsei experience of 5000 gasless transaxillary robotic thyroidectomies. World J Surg. 2018; Feb. 42(2):393–401.19. Terris DJ, Singer MC, Seybt MW. Robotic facelift thyroidectomy: II. Clinical feasibility and safety. Laryngoscope. 2011; Aug. 121(8):1636–41.20. Richmon JD, Kim HY. Transoral robotic thyroidectomy (TORT): procedures and outcomes. Gland Surg. 2017; Jun. 6(3):285–9.21. Seong CY, Yu HW, Chai YJ, Lee KE. Oncoplastic thyroid surgery using a bilateral axillo-breast approach. J Minim Invasive Surg. 2017; 20(2):51–7.22. Kwak J, Yu HW, Ahn JH, Kim SJ, Chai YJ, Choi JY, et al. A time trend analysis of 5,000 robotic thyroidectomies via bilateral axillo-breast approach. World J Surg. 2023; Feb. 47(2):403–11.23. Kwon H, Yi JW, Song RY, Chai YJ, Kim SJ, Choi JY, et al. Comparison of bilateral axillo-breast approach robotic thyroidectomy with open thyroidectomy for Graves’ disease. World J Surg. 2016; Mar. 40(3):498–504.24. Chai YJ, Suh H, Woo JW, Yu HW, Song RY, Kwon H, et al. Surgical safety and oncological completeness of robotic thyroidectomy for thyroid carcinoma larger than 2 cm. Surg Endosc. 2017; Mar. 31(3):1235–40.25. Yu HW, Chai YJ, Kim SJ, Choi JY, Lee KE. Robotic-assisted modified radical neck dissection using a bilateral axillo-breast approach (robotic BABA MRND) for papillary thyroid carcinoma with lateral lymph node metastasis. Surg Endosc. 2018; May. 32(5):2322–7.26. Lee KE, Koo do H, Im HJ, Park SK, Choi JY, Paeng JC, et al. Surgical completeness of bilateral axillo-breast approach robotic thyroidectomy: comparison with conventional open thyroidectomy after propensity score matching. Surgery. 2011; Dec. 150(6):1266–74.27. Kim W, Lee JK, Choi JH, Yu HW, Kim Sj, Chai YJ, et al. Reduced port robotic bilateral axillo-breast approach (BABA) isthmusectomy. J Endocr Surg. 2021; 21(4):111–7.28. Yoon HJ, Ahn JH, Kim JH, Yi JW, Hur MH. Initial experience of BABA robotic thyroidectomy using the Da Vinci Xi system in Incheon, Korea. J Endocr Surg. 2019; 19(3):59–67.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Retroauricular Thyroidectomy Using a New Flexible, Single-Port Robotic Surgical System
- Robotic Transoral Thyroidectomy: Right Thyroidectomy and Ipsilateral Central Neck Dissection with da Vinci Si Surgical System
- Single-port plus an additional port robotic complete mesocolic excision and intracorporeal anastomosis using a robotic stapler for right-sided colon cancer
- Bilateral axillo-breast approach robotic total thyroidectomy without isthmectomy: a case report
- Single-Port Transaxillary Robotic Thyroidectomy (START) for Benign Thyroid Tumors
