J Yeungnam Med Sci.
2023 Jul;40(3):297-301. 10.12701/jyms.2022.00591.
Effect of pulmonary rehabilitation on patients with acute COVID-19: a single-center case series
- Affiliations
-
- 1Department of Physical Medicine and Rehabilitation, Seoul Medical Center, Seoul, Korea
- KMID: 2544592
- DOI: http://doi.org/10.12701/jyms.2022.00591
Abstract
- The coronavirus disease 2019 (COVID-19) pandemic has been ongoing for more than 2 years. Many patients who recover from severe acute respiratory syndrome coronavirus 2 infection continue to have aftereffects such as dyspnea and fatigue, which may lead to functional decline. Therefore, the need for managing these symptoms using methods such as pulmonary rehabilitation (PR) has emerged. The purpose of this study was to report the effectiveness of PR in five patients with acute COVID-19. PR was performed in patients with persistent dyspnea and oxygen demand after COVID-19. All five patients were able to maintain an independent functional status before COVID-19. However, after acute COVID-19, they were unable to walk independently and needed assistance for activities of daily living due to dyspnea and fatigue. Therefore, they were referred to rehabilitation units, and PR was performed. The modified Medical Research Council dyspnea scale, maximal expiratory pressure (MEP), 6-minute walking test, forced vital capacity, and grip strength were assessed before and after PR, and the results were compared. After PR, the parameters improved, except for the MEP in one patient (patient 3) and the grip strength in another patient (patient 4). After PR, two out of five patients returned to work and the other three returned home. Therefore, we conclude that PR is necessary for patients with acute COVID-19 with activity limitations.
Keyword
Figure
-
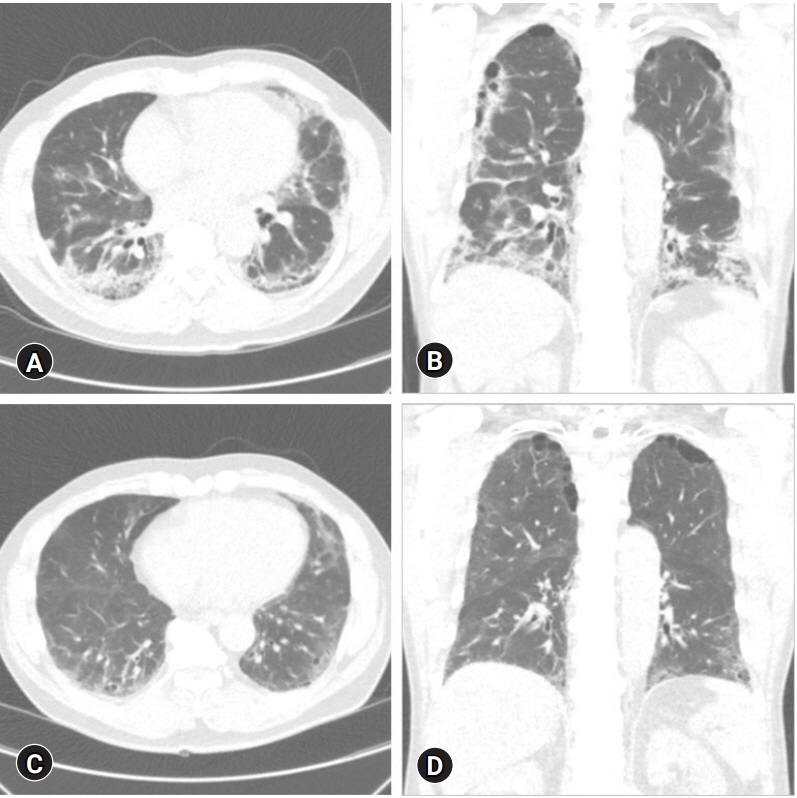
Fig. 1. Chest computed tomography of patient 2. (A) Axial view and (B) coronal view (before pulmonary rehabilitation [PR]). Ground glass opacities and pulmonary fibrosis are present in both lungs. (C) Axial view and (D) coronal view (4-month follow-up after PR). Ground-glass opacities and pulmonary fibrosis of both lungs decreased compared to panels A and B.
Reference
-
References
1. Datta SD, Talwar A, Lee JT. A proposed framework and timeline of the spectrum of disease due to SARS-CoV-2 infection: illness beyond acute infection and public health implications. JAMA. 2020; 324:2251–2.2. Greenhalgh T, Knight M, A’Court C, Buxton M, Husain L. Management of post-acute covid-19 in primary care. BMJ. 2020; 370:m3026.3. Montani D, Savale L, Noel N, Meyrignac O, Colle R, Gasnier M, et al. Post-acute COVID-19 syndrome. Eur Respir Rev. 2022; 31:210185.4. Nalbandian A, Sehgal K, Gupta A, Madhavan MV, McGroder C, Stevens JS, et al. Post-acute COVID-19 syndrome. Nat Med. 2021; 27:601–15.5. Spruit MA, Holland AE, Singh SJ, Tonia T, Wilson KC, Troosters T. COVID-19: interim guidance on rehabilitation in the hospital and post-hospital phase from a European Respiratory Society- and American Thoracic Society-coordinated international task force. Eur Respir J. 2020; 56:2002197.6. Evans JA, Whitelaw WA. The assessment of maximal respiratory mouth pressures in adults. Respir Care. 2009; 54:1348–59.7. ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: guidelines for the six-minute walk test. Am J Respir Crit Care Med. 2002; 166:111–7.8. Massy-Westropp NM, Gill TK, Taylor AW, Bohannon RW, Hill CL. Hand grip strength: age and gender stratified normative data in a population-based study. BMC Res Notes. 2011; 4:127.9. Bohannon RW. Muscle strength: clinical and prognostic value of hand-grip dynamometry. Curr Opin Clin Nutr Metab Care. 2015; 18:465–70.10. Lechowicz K, Drożdżal S, Machaj F, Rosik J, Szostak B, Zegan-Barańska M, et al. COVID-19: the potential treatment of pulmonary fibrosis associated with SARS-CoV-2 infection. J Clin Med. 2020; 9:1917.11. Lee AL, Hill CJ, McDonald CF, Holland AE. Pulmonary rehabilitation in individuals with non-cystic fibrosis bronchiectasis: a systematic review. Arch Phys Med Rehabil. 2017; 98:774–82.e1.12. Jimeno-Almazán A, Pallarés JG, Buendía-Romero Á, Martínez-Cava A, Franco-López F, Sánchez-Alcaraz Martínez BJ, et al. Post-COVID-19 syndrome and the potential benefits of exercise. Int J Environ Res Public Health. 2021; 18:5329.13. Nici L, Donner C, Wouters E, Zuwallack R, Ambrosino N, Bourbeau J, et al. American Thoracic Society/European Respiratory Society statement on pulmonary rehabilitation. Am J Respir Crit Care Med. 2006; 173:1390–413.14. Kurtaiş Aytür Y, Köseoğlu BF, Özyemişçi Taşkıran Ö, Ordu-Gökkaya NK, Ünsal Delialioğlu S, Sonel Tur B, et al. Pulmonary rehabilitation principles in SARS-COV-2 infection (COVID-19): a guideline for the acute and subacute rehabilitation. Turk J Phys Med Rehabil. 2020; 66:104–20.15. Severin R, Arena R, Lavie CJ, Bond S, Phillips SA. Respiratory muscle performance screening for infectious disease management following COVID-19: a highly pressurized situation. Am J Med. 2020; 133:1025–32.16. Jacobs LG, Gourna Paleoudis E, Lesky-Di Bari D, Nyirenda T, Friedman T, Gupta A, et al. Persistence of symptoms and quality of life at 35 days after hospitalization for COVID-19 infection. PLoS One. 2020; 15:e0243882.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- New-Onset Seizures in Patients With COVID-19: A Case Series From a Single Public Hospital in Korea
- An unusual presentation of COVID-19: Acute pancreatitis
- Post–Coronavirus Disease 2019 Pulmonary Fibrosis: Wait or Needs Intervention
- Post-COVID-19 Syndrome
- Pulmonary Contusion Similar to COVID-19 Pneumonia
