Utility of narrow-band imaging with or without dual focus magnification in neoplastic prediction of small colorectal polyps: a Vietnamese experience
- Affiliations
-
- 1Department of Internal Medicine, University of Medicine and Pharmacy at Hochiminh City, Ho Chi Minh City, Vietnam
- 2Department of Endoscopy, University Medical Center, Ho Chi Minh City, Vietnam
- 3Department of Surgical Pathology, University of Medicine and Pharmacy at Hochiminh City, Ho Chi Minh City, Vietnam
- KMID: 2544571
- DOI: http://doi.org/10.5946/ce.2022.212
Abstract
- Background/Aims
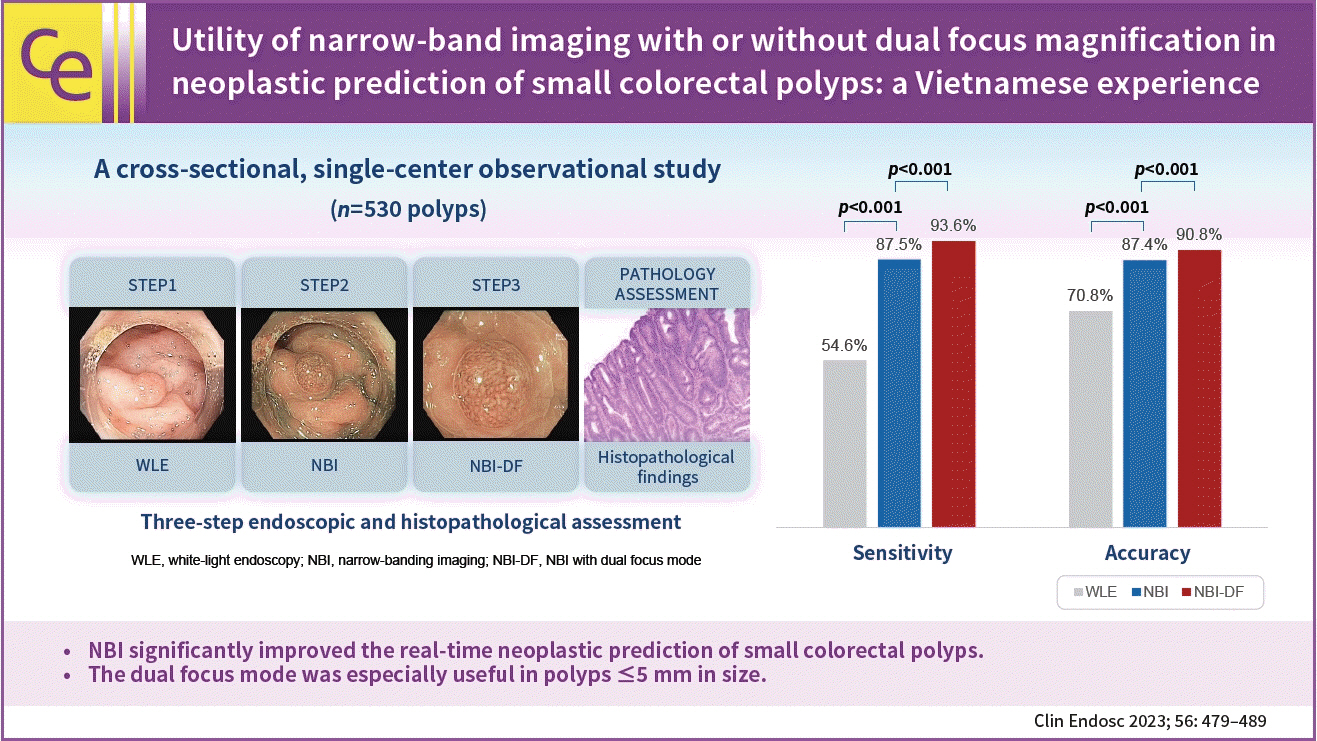
Accurate neoplastic prediction can significantly decrease costs associated with pathology and unnecessary colorectal polypectomies. Narrow band imaging (NBI) and dual-focus (DF) mode are promising emerging optical technologies for recognizing neoplastic features of colorectal polyps digitally. This study aimed to clarify the clinical usefulness of NBI with and without DF assistance in the neoplastic prediction of small colorectal polyps (<10 mm).
Methods
This cross-sectional study included 530 small colorectal polyps from 343 consecutive patients who underwent colonoscopy at the University Medical Center from September 2020 to May 2021. Each polyp was endoscopically diagnosed in three successive steps using white-light endoscopy (WLE), NBI, and NBI-DF and retrieved for histopathological assessment. The diagnostic accuracy of each modality was evaluated with reference to histopathology.
Results
There were 295 neoplastic polyps and 235 non-neoplastic polyps. The overall accuracies of WLE, WLE+NBI, and WLE+NBI+NBI-DF in the neoplastic prediction of colorectal polyps were 70.8%, 87.4%, and 90.8%, respectively (p<0.001). The accuracy of WLE+NBI+NBI-DF was significantly higher than that of WLE+NBI in the polyp size ≤5 mm subgroup (87.3% vs. 90.1%, p<0.001).
Conclusions
NBI improved the real-time neoplastic prediction of small colorectal polyps. The DF mode was especially useful in polyps ≤5 mm in size.
Figure
-
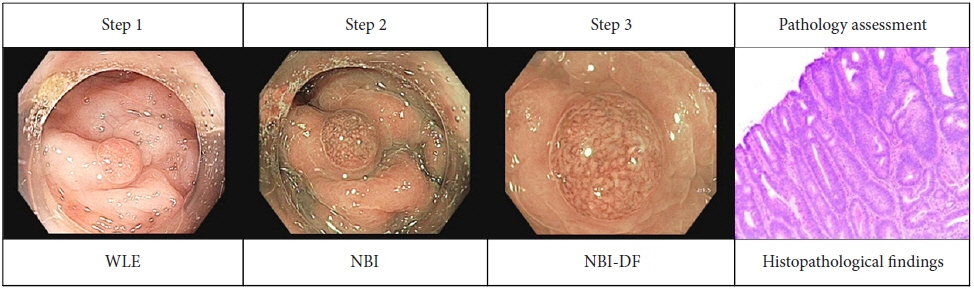
Fig. 1. Illustration of endoscopic and histopathological assessment. WLE, white-light endoscopy; NBI, narrow-band imaging; NBI-DF, NBI with dual-focus.
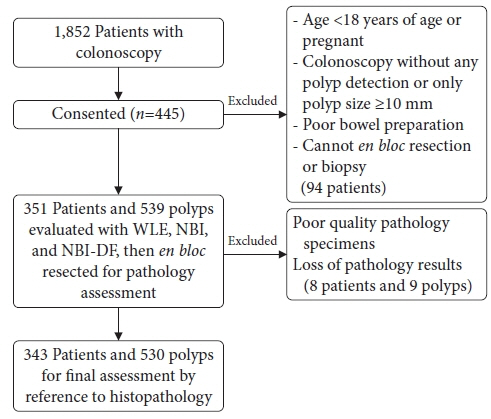
Fig. 2. Study flowchart. WLE, white-light endoscopy; NBI, narrow-band imaging; NBI-DF, NBI with dual-focus.
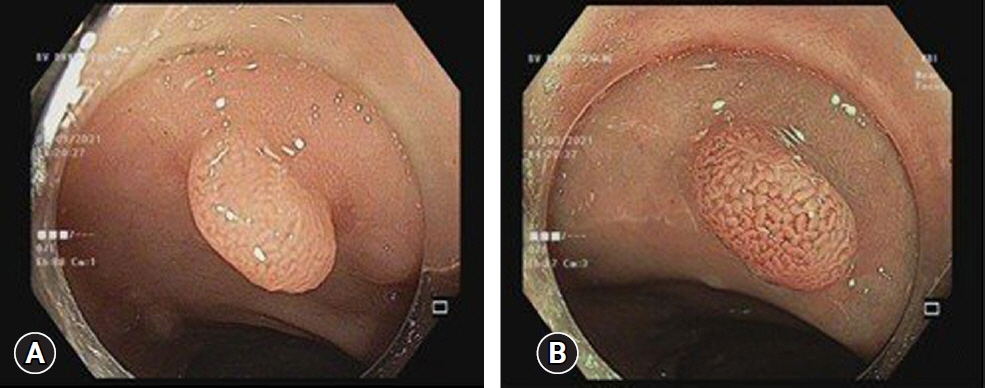
Fig. 3. A sessile-type lesion (0–Is), 7 mm in size, had tubulogyrus patterns in white-light endoscopy (A) and was subsequently classified as NICE 2 by narrow-band imaging with dual-focus (B). Histology revealed a tubular adenoma with low-grade dysplasia.
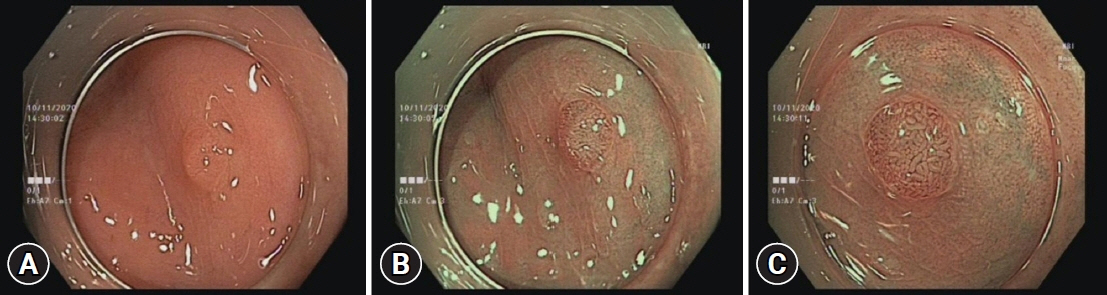
Fig. 4. A flat-type lesion (0 – IIa), 5 mm in size. White-light endoscopy showed a 0-IIa, 4 mm lesion with non-neoplastic characteristics and the same color as the background (A). After adding narrow-band imaging (NBI), a light brown lesion was classified as NICE 2 with low confidence, since the polyp size limited the evaluation the surface and vessel pattern (B). Subsequently, the lesion was classified as NICE 2 with high confidence by NBI with dual-focus magnification (C). Final histological findings revealed a tubular adenoma with low-grade dysplasia.
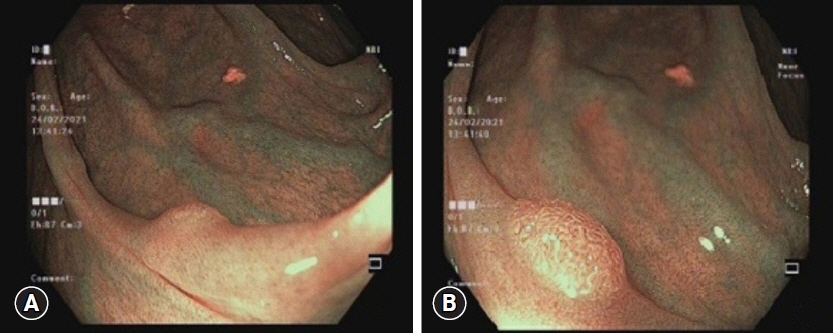
Fig. 5. Hyperplastic polyps contained blood vessels that appeared similar to the meshed capillary network observed in neoplastic lesions. (A) Narrow-band imaging (NBI). (B) NBI with dual-focus. The histology results indicated a hyperplastic polyp.

Fig. 6. The lesion had a dark and brown surface with an atypical capillary pattern in white-light endoscopy (A) and narrow-band imaging (NBI) with dual-focus (B). These led to misclassification as NICE 2; the final histology result was an inflammatory polyp.
Reference
-
1. Winawer SJ, Zauber AG, O’Brien MJ, et al. Randomized comparison of surveillance intervals after colonoscopic removal of newly diagnosed adenomatous polyps. The National Polyp Study Workgroup. N Engl J Med. 1993; 328:901–906.2. Zauber AG, Winawer SJ, O’Brien MJ, et al. Colonoscopic polypectomy and long-term prevention of colorectal-cancer deaths. N Engl J Med. 2012; 366:687–696.3. Ponugoti PL, Cummings OW, Rex DK. Risk of cancer in small and diminutive colorectal polyps. Dig Liver Dis. 2017; 49:34–37.4. Iwatate M, Ikumoto T, Hattori S, et al. NBI and NBI combined with magnifying colonoscopy. Diagn Ther Endosc. 2012; 2012:173269.5. Hewett DG, Kaltenbach T, Sano Y, et al. Validation of a simple classification system for endoscopic diagnosis of small colorectal polyps using narrow-band imaging. Gastroenterology. 2012; 143:599–607.6. Ciocâlteu AM, CârŢână ET, Florescu DN, et al. Narrow band imaging with near-focus mode for colorectal polyps’ characterization. Rom J Morphol Embryol. 2016; 57(2 Suppl):619–626.7. Iwatate M, Sano Y, Hattori S, et al. The addition of high magnifying endoscopy improves rates of high confidence optical diagnosis of colorectal polyps. Endosc Int Open. 2015; 3:E140–E145.8. Ikematsu H, Matsuda T, Osera S, et al. Usefulness of narrow-band imaging with dual-focus magnification for differential diagnosis of small colorectal polyps. Surg Endosc. 2015; 29:844–850.9. Rex DK. Narrow-band imaging without optical magnification for histologic analysis of colorectal polyps. Gastroenterology. 2009; 136:1174–1181.10. Rastogi A, Keighley J, Singh V, et al. High accuracy of narrow band imaging without magnification for the real-time characterization of polyp histology and its comparison with high-definition white light colonoscopy: a prospective study. Am J Gastroenterol. 2009; 104:2422–2430.11. Chiu HM, Chang CY, Chen CC, et al. A prospective comparative study of narrow-band imaging, chromoendoscopy, and conventional colonoscopy in the diagnosis of colorectal neoplasia. Gut. 2007; 56:373–379.12. Kuruvilla N, Paramsothy R, Gill R, et al. A prospective dual-center proof-of-principle study evaluating the incremental benefit of narrow-band imaging with a fixed zoom function in real-time prediction of polyp histology: can we resect and discard? Gastrointest Endosc. 2015; 82:362–369.13. The Paris endoscopic classification of superficial neoplastic lesions: esophagus, stomach, and colon: November 30 to December 1, 2002. Gastrointest Endosc. 2003; 58(6 Suppl):S3–43.14. Singh R, Bhat YM, Thurairajah PH, et al. Is narrow band imaging superior to high-definition white light endoscopy in the assessment of diminutive colorectal polyps? J Gastroenterol Hepatol. 2013; 28:472–478.15. Nagtegaal ID, Odze RD, Klimstra D, et al. The 2019 WHO classification of tumours of the digestive system. Histopathology. 2020; 76:182–188.16. McGill SK, Evangelou E, Ioannidis JP, et al. Narrow band imaging to differentiate neoplastic and non-neoplastic colorectal polyps in real time: a meta-analysis of diagnostic operating characteristics. Gut. 2013; 62:1704–1713.17. Kaltenbach T, Rastogi A, Rouse RV, et al. Real-time optical diagnosis for diminutive colorectal polyps using narrow-band imaging: the VALID randomised clinical trial. Gut. 2015; 64:1569–1577.18. Hattori S, Iwatate M, Sano W, et al. Narrow-band imaging observation of colorectal lesions using NICE classification to avoid discarding significant lesions. World J Gastrointest Endosc. 2014; 6:600–605.19. Szura M, Pasternak A, Bucki K, et al. Two-stage optical system for colorectal polyp assessments. Surg Endosc. 2016; 30:204–214.20. Wallace MB, Crook JE, Coe S, et al. Accuracy of in vivo colorectal polyp discrimination by using dual-focus high-definition narrow-band imaging colonoscopy. Gastrointest Endosc. 2014; 80:1072–1087.21. Singh R, Jayanna M, Navadgi S, et al. Narrow-band imaging with dual focus magnification in differentiating colorectal neoplasia. Dig Endosc. 2013; 25 Suppl 2:16–20.22. Higashi R, Uraoka T, Kato J, et al. Diagnostic accuracy of narrow-band imaging and pit pattern analysis significantly improved for less-experienced endoscopists after an expanded training program. Gastrointest Endosc. 2010; 72:127–135.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Randomized Controlled Clinical Study Comparing the Diagnostic Accuracy of the Histologic Prediction for Colorectal Polyps Depending on the Use of Either Magnified or Nonmagnified Narrow Band Imaging
- Optical diagnosis by near-focus versus normal-focus narrow band imaging colonoscopy in colorectal polyps based on combined NICE and WASP classification: a randomized controlled trial
- Optical Diagnosis for Colorectal Polyps: A Useful Technique Now or in the Future?
- Polyp Detection, Characterization, and Management Using Narrow-Band Imaging with/without Magnification
- Correlation of Narrow Band Imaging with Magnifying Colonoscopy and Histology in Colorectal Tumors
