Complications of endoscopic resection in the upper gastrointestinal tract
- Affiliations
-
- 1Endoscopy Division, National Cancer Center Hospital, Tokyo, Japan
- KMID: 2544562
- DOI: http://doi.org/10.5946/ce.2023.024
Abstract
- Endoscopic resection (ER) is widely utilized as a minimally invasive treatment for upper gastrointestinal tumors; however, complications could occur during and after the procedure. Post-ER mucosal defect leads to delayed perforation and bleeding; therefore, endoscopic closure methods (endoscopic hand-suturing, the endoloop and endoclip closure method, and over-the-scope clip method) and tissue shielding methods (polyglycolic acid sheets and fibrin glue) are developed to prevent these complications. During duodenal ER, complete closure of the mucosal defect significantly reduces delayed bleeding and should be performed. An extensive mucosal defect that comprises three-quarters of the circumference in the esophagus, gastric antrum, or cardia is a significant risk factor for post-ER stricture. Steroid therapy is considered the first-line option for the prevention of esophageal stricture, but its efficacy for gastric stricture remains unclear. Methods for the prevention and management of ER-related complications in the esophagus, stomach, and duodenum differ according to the organ; therefore, endoscopists should be familiar with ways of preventing and managing organ-specific complications.
Figure
-

Fig. 1. Tissue shielding method with polyglycolic acid sheet and fibrin glue. (A) A 15-mm type 0–IIc lesion was located in the lesser curvature of the pyloric ring. (B) Endoscopic submucosal dissection (ESD) was performed, and en bloc resection was achieved. (C) Polyglycolic acid sheet and fibrin glue were attached to the post-ESD ulcer. (D) Postoperative day (POD) 5. (E) POD 15. (F) POD 60. There were no adverse events after the ESD.
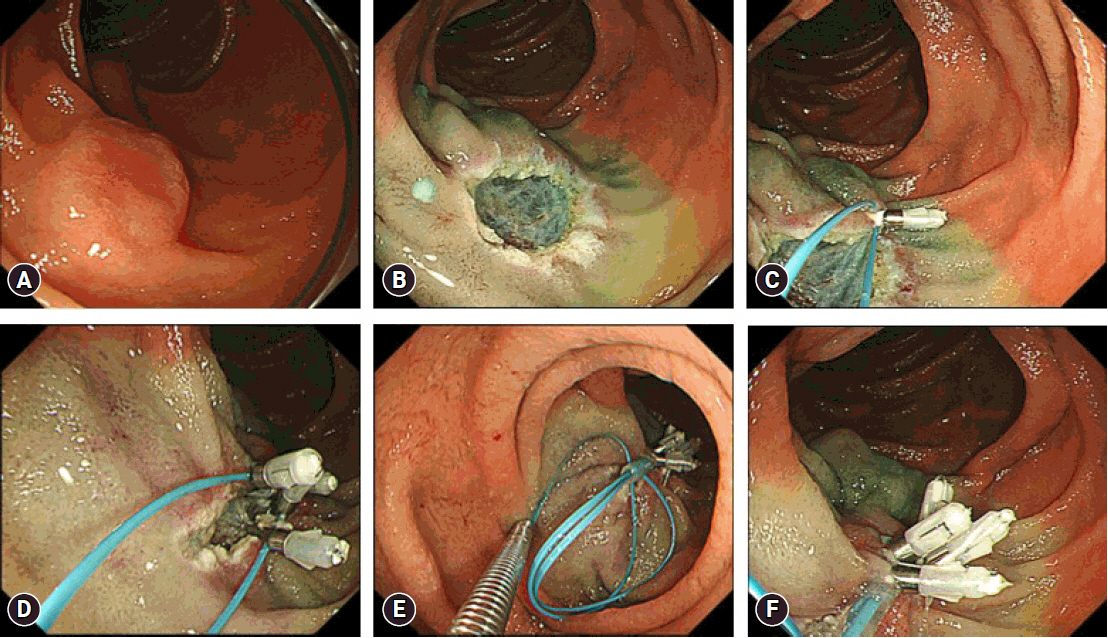
Fig. 2. Endoloop and endoclip closure method. (A) A 12-mm type 0–IIa lesion was located in the second part of the duodenum. (B) Endoscopic mucosal resection was performed, and en bloc resection was achieved. (C) The endoloop was anchored to the distal side of the mucosal defect. (D) The endloop was placed with the endoclips along the edge of the mucosal defect. (E) The mucosal defect was closed by tightening the fixed endoloop. (F) Complete closure was successfully achieved.
Reference
-
1. Yamashina T, Ishihara R, Nagai K, et al. Long-term outcome and metastatic risk after endoscopic resection of superficial esophageal squamous cell carcinoma. Am J Gastroenterol. 2013; 108:544–551.2. Tanabe S, Ishido K, Matsumoto T, et al. Long-term outcomes of endoscopic submucosal dissection for early gastric cancer: a multicenter collaborative study. Gastric Cancer. 2017; 20(Suppl 1):45–52.3. Berger A, Rahmi G, Perrod G, et al. Long-term follow-up after endoscopic resection for superficial esophageal squamous cell carcinoma: a multicenter Western study. Endoscopy. 2019; 51:298–306.4. Yeh JH, Huang RY, Lee CT, et al. Long-term outcomes of endoscopic submucosal dissection and comparison to surgery for superficial esophageal squamous cancer: a systematic review and meta-analysis. Therap Adv Gastroenterol. 2020; 13:1756284820964316.5. Abdelfatah MM, Barakat M, Ahmad D, et al. Long-term outcomes of endoscopic submucosal dissection versus surgery in early gastric cancer: a systematic review and meta-analysis. Eur J Gastroenterol Hepatol. 2019; 31:418–424.6. Nonaka S, Oda I, Tada K, et al. Clinical outcome of endoscopic resection for nonampullary duodenal tumors. Endoscopy. 2015; 47:129–135.7. Suzuki H, Ono H, Hirasawa T, et al. Long-term survival after endoscopic resection for gastric cancer: real-world evidence from a multicenter prospective cohort. Clin Gastroenterol Hepatol. 2023; 21:307–318.8. Oyama T, Tomori A, Hotta K, et al. Endoscopic submucosal dissection of early esophageal cancer. Clin Gastroenterol Hepatol. 2005; 3(7 Suppl 1):S67–S70.9. Ishihara R, Iishi H, Uedo N, et al. Comparison of EMR and endoscopic submucosal dissection for en bloc resection of early esophageal cancers in Japan. Gastrointest Endosc. 2008; 68:1066–1072.10. Oka S, Tanaka S, Kaneko I, et al. Advantage of endoscopic submucosal dissection compared with EMR for early gastric cancer. Gastrointest Endosc. 2006; 64:877–883.11. Park YM, Cho E, Kang HY, et al. The effectiveness and safety of endoscopic submucosal dissection compared with endoscopic mucosal resection for early gastric cancer: a systematic review and metaanalysis. Surg Endosc. 2011; 25:2666–2677.12. Nakamoto S, Sakai Y, Kasanuki J, et al. Indications for the use of endoscopic mucosal resection for early gastric cancer in Japan: a comparative study with endoscopic submucosal dissection. Endoscopy. 2009; 41:746–750.13. Lian J, Chen S, Zhang Y, et al. A meta-analysis of endoscopic submucosal dissection and EMR for early gastric cancer. Gastrointest Endosc. 2012; 76:763–770.14. Cao Y, Liao C, Tan A, et al. Meta-analysis of endoscopic submucosal dissection versus endoscopic mucosal resection for tumors of the gastrointestinal tract. Endoscopy. 2009; 41:751–757.15. Suzuki H, Takizawa K, Hirasawa T, et al. Short-term outcomes of multicenter prospective cohort study of gastric endoscopic resection: ‘real-world evidence’ in Japan. Dig Endosc. 2019; 31:30–39.16. Ishihara R, Arima M, Iizuka T, et al. Endoscopic submucosal dissection/endoscopic mucosal resection guidelines for esophageal cancer. Dig Endosc. 2020; 32:452–493.17. Guo HM, Zhang XQ, Chen M, et al. Endoscopic submucosal dissection vs endoscopic mucosal resection for superficial esophageal cancer. World J Gastroenterol. 2014; 20:5540–5547.18. Furue Y, Katada C, Tanabe S, et al. Effectiveness and safety of endoscopic aspiration mucosectomy and endoscopic submucosal dissection in patients with superficial esophageal squamous-cell carcinoma. Surg Endosc. 2019; 33:1433–1440.19. Fujishiro M, Yahagi N, Kakushima N, et al. Endoscopic submucosal dissection of esophageal squamous cell neoplasms. Clin Gastroenterol Hepatol. 2006; 4:688–694.20. Takahashi H, Arimura Y, Masao H, et al. Endoscopic submucosal dissection is superior to conventional endoscopic resection as a curative treatment for early squamous cell carcinoma of the esophagus (with video). Gastrointest Endosc. 2010; 72:255–264.21. Teoh AY, Chiu PW, Yu Ngo DK, et al. Outcomes of endoscopic submucosal dissection versus endoscopic mucosal resection in management of superficial squamous esophageal neoplasms outside Japan. J Clin Gastroenterol. 2010; 44:e190–e194.22. Tsujii Y, Nishida T, Nishiyama O, et al. Clinical outcomes of endoscopic submucosal dissection for superficial esophageal neoplasms: a multicenter retrospective cohort study. Endoscopy. 2015; 47:775–783.23. Odagiri H, Yasunaga H, Matsui H, et al. Hospital volume and adverse events following esophageal endoscopic submucosal dissection in Japan. Endoscopy. 2017; 49:321–326.24. Koyama Y, Abe S, Itoi T. Extensive perforation of the esophagus caused by a localized muscle layer defect during endoscopic submucosal dissection. Dig Endosc. 2022; 34:e40–e41.25. Abe S, Wu SY, Ego M, et al. Efficacy of current traction techniques for endoscopic submucosal dissection. Gut Liver. 2020; 14:673–684.26. Yoshida M, Takizawa K, Nonaka S, et al. Conventional versus traction-assisted endoscopic submucosal dissection for large esophageal cancers: a multicenter, randomized controlled trial (with video). Gastrointest Endosc. 2020; 91:55–65.27. Yamamoto Y, Kikuchi D, Nagami Y, et al. Management of adverse events related to endoscopic resection of upper gastrointestinal neoplasms: review of the literature and recommendations from experts. Dig Endosc. 2019; 31 Suppl 1:4–20.28. Lee JH, Kedia P, Stavropoulos SN, et al. AGA clinical practice update on endoscopic management of perforations in gastrointestinal tract: expert review. Clin Gastroenterol Hepatol. 2021; 19:2252–2261.29. Takahashi R, Yoshio T, Horiuchi Y, et al. Endoscopic tissue shielding for esophageal perforation caused by endoscopic resection. Clin J Gastroenterol. 2017; 10:214–219.30. Seehawong U, Morita Y, Nakano Y, et al. Successful treatment of an esophageal perforation that occurred during endoscopic submucosal dissection for esophageal cancer using polyglycolic acid sheets and fibrin glue. Clin J Gastroenterol. 2019; 12:29–33.31. Omae M, Konradsson M, Baldaque-Silva F. Delayed perforation after endoscopic submucosal dissection treated successfully by temporary stent placement. Clin J Gastroenterol. 2018; 11:118–122.32. Matsuda Y, Kataoka N, Yamaguchi T, et al. Delayed esophageal perforation occurring with endoscopic submucosal dissection: a report of two cases. World J Gastrointest Surg. 2015; 7:123–127.33. Urabe Y, Hiyama T, Tanaka S, et al. Advantages of endoscopic submucosal dissection versus endoscopic oblique aspiration mucosectomy for superficial esophageal tumors. J Gastroenterol Hepatol. 2011; 26:275–280.34. Shi Q, Ju H, Yao LQ, et al. Risk factors for postoperative stricture after endoscopic submucosal dissection for superficial esophageal carcinoma. Endoscopy. 2014; 46:640–644.35. Katada C, Muto M, Manabe T, et al. Esophageal stenosis after endoscopic mucosal resection of superficial esophageal lesions. Gastrointest Endosc. 2003; 57:165–169.36. Ono S, Fujishiro M, Niimi K, et al. Predictors of postoperative stricture after esophageal endoscopic submucosal dissection for superficial squamous cell neoplasms. Endoscopy. 2009; 41:661–665.37. Wen J, Lu Z, Yang Y, et al. Preventing stricture formation by covered esophageal stent placement after endoscopic submucosal dissection for early esophageal cancer. Dig Dis Sci. 2014; 59:658–663.38. Hanaoka N, Ishihara R, Takeuchi Y, et al. Intralesional steroid injection to prevent stricture after endoscopic submucosal dissection for esophageal cancer: a controlled prospective study. Endoscopy. 2012; 44:1007–1011.39. Yamaguchi N, Isomoto H, Nakayama T, et al. Usefulness of oral prednisolone in the treatment of esophageal stricture after endoscopic submucosal dissection for superficial esophageal squamous cell carcinoma. Gastrointest Endosc. 2011; 73:1115–1121.40. Tanaka M, Ono H, Takizawa K. A randomized controlled phase III trial comparing oral prednisolone administration and local triamcinolone injection therapy for the prevention of esophageal stricture after endoscopic submucosal dissection, JCOG 1217 (Abstract). United European Gastroenterol J. 2022; 10(suppl 8):9–184.41. Chu Y, Chen T, Li H, et al. Long-term efficacy and safety of intralesional steroid injection plus oral steroid administration in preventing stricture after endoscopic submucosal dissection for esophageal epithelial neoplasms. Surg Endosc. 2019; 33:1244–1251.42. Sakaguchi Y, Tsuji Y, Shinozaki T, et al. Steroid injection and polyglycolic acid shielding to prevent stricture after esophageal endoscopic submucosal dissection: a retrospective comparative analysis (with video). Gastrointest Endosc. 2020; 92:1176–1186.43. Ohki T, Yamato M, Ota M, et al. Prevention of esophageal stricture after endoscopic submucosal dissection using tissue-engineered cell sheets. Gastroenterology. 2012; 143:582–588.44. Ohki T, Yamato M, Ota M, et al. Application of regenerative medical technology using tissue-engineered cell sheets for endoscopic submucosal dissection of esophageal neoplasms. Dig Endosc. 2015; 27:182–188.45. Ezoe Y, Muto M, Horimatsu T, et al. Efficacy of preventive endoscopic balloon dilation for esophageal stricture after endoscopic resection. J Clin Gastroenterol. 2011; 45:222–227.46. Nonaka K, Miyazawa M, Ban S, et al. Different healing process of esophageal large mucosal defects by endoscopic mucosal dissection between with and without steroid injection in an animal model. BMC Gastroenterol. 2013; 13:72.47. Kadota T, Yano T, Kato T, et al. Prophylactic steroid administration for strictures after endoscopic resection of large superficial esophageal squamous cell carcinoma. Endosc Int Open. 2016; 4:E1267–E1274.48. Sakaguchi Y, Tsuji Y, Fujishiro M, et al. Triamcinolone injection and shielding with polyglycolic acid sheets and fibrin glue for postoperative stricture prevention after esophageal endoscopic resection: a pilot study. Am J Gastroenterol. 2016; 111:581–583.49. Sakaguchi Y, Tsuji Y, Ono S, et al. Polyglycolic acid sheets with fibrin glue can prevent esophageal stricture after endoscopic submucosal dissection. Endoscopy. 2015; 47:336–340.50. Yoda Y, Yano T, Kaneko K, et al. Endoscopic balloon dilatation for benign fibrotic strictures after curative nonsurgical treatment for esophageal cancer. Surg Endosc. 2012; 26:2877–2883.51. Takahashi H, Arimura Y, Okahara S, et al. Risk of perforation during dilation for esophageal strictures after endoscopic resection in patients with early squamous cell carcinoma. Endoscopy. 2011; 43:184–189.52. Kishida Y, Kakushima N, Kawata N, et al. Complications of endoscopic dilation for esophageal stenosis after endoscopic submucosal dissection of superficial esophageal cancer. Surg Endosc. 2015; 29:2953–2959.53. Tsujii Y, Hayashi Y, Kawai N, et al. Risk of perforation in balloon dilation associated with steroid injection for preventing esophageal stricture after endoscopic submucosal dissection. Endosc Int Open. 2017; 5:E573–E579.54. Muto M, Ezoe Y, Yano T, et al. Usefulness of endoscopic radial incision and cutting method for refractory esophagogastric anastomotic stricture (with video). Gastrointest Endosc. 2012; 75:965–972.55. Ono H, Yao K, Fujishiro M, et al. Guidelines for endoscopic submucosal dissection and endoscopic mucosal resection for early gastric cancer (second edition). Dig Endosc. 2021; 33:4–20.56. Ikehara H, Gotoda T, Ono H, et al. Gastric perforation during endoscopic resection for gastric carcinoma and the risk of peritoneal dissemination. Br J Surg. 2007; 94:992–995.57. Minami S, Gotoda T, Ono H, et al. Complete endoscopic closure of gastric perforation induced by endoscopic resection of early gastric cancer using endoclips can prevent surgery (with video). Gastrointest Endosc. 2006; 63:596–601.58. Abe S, Oda I, Mori G, et al. Complete endoscopic closure of a large gastric defect with endoloop and endoclips after complex endoscopic submucosal dissection. Endoscopy. 2015; 47 Suppl 1 UCTN:E374–E375.59. Kobara H, Mori H, Nishiyama N, et al. Over-the-scope clip system: a review of 1517 cases over 9 years. J Gastroenterol Hepatol. 2019; 34:22–30.60. Nagami Y, Shiba M, Arakawa T. Use of PGA sheets in the endoscopic closure of a perforation after endoscopic submucosal dissection for gastric-tube cancer. Am J Gastroenterol. 2016; 111:768.61. Jeong JY, Oh YH, Yu YH, et al. Does submucosal fibrosis affect the results of endoscopic submucosal dissection of early gastric tumors? Gastrointest Endosc. 2012; 76:59–66.62. Ohta T, Ishihara R, Uedo N, et al. Factors predicting perforation during endoscopic submucosal dissection for gastric cancer. Gastrointest Endosc. 2012; 75:1159–1165.63. Yoshida M, Takizawa K, Suzuki S, et al. Conventional versus traction-assisted endoscopic submucosal dissection for gastric neoplasms: a multicenter, randomized controlled trial (with video). Gastrointest Endosc. 2018; 87:1231–1240.64. Suzuki H, Oda I, Sekiguchi M, et al. Management and associated factors of delayed perforation after gastric endoscopic submucosal dissection. World J Gastroenterol. 2015; 21:12635–12643.65. Hanaoka N, Uedo N, Ishihara R, et al. Clinical features and outcomes of delayed perforation after endoscopic submucosal dissection for early gastric cancer. Endoscopy. 2010; 42:1112–1115.66. Kang SH, Lee K, Lee HW, et al. Delayed perforation occurring after endoscopic submucosal dissection for early gastric cancer. Clin Endosc. 2015; 48:251–255.67. Ono H, Takizawa K, Kakushima N, et al. Application of polyglycolic acid sheets for delayed perforation after endoscopic submucosal dissection of early gastric cancer. Endoscopy. 2015; 47 Suppl 1 UCTN:E18–E19.68. Ikezawa K, Michida T, Iwahashi K, et al. Delayed perforation occurring after endoscopic submucosal dissection for early gastric cancer. Gastric Cancer. 2012; 15:111–114.69. Takizawa K, Oda I, Gotoda T, et al. Routine coagulation of visible vessels may prevent delayed bleeding after endoscopic submucosal dissection: an analysis of risk factors. Endoscopy. 2008; 40:179–183.70. Uedo N, Takeuchi Y, Yamada T, et al. Effect of a proton pump inhibitor or an H2-receptor antagonist on prevention of bleeding from ulcer after endoscopic submucosal dissection of early gastric cancer: a prospective randomized controlled trial. Am J Gastroenterol. 2007; 102:1610–1616.71. Yang Z, Wu Q, Liu Z, et al. Proton pump inhibitors versus histamine-2-receptor antagonists for the management of iatrogenic gastric ulcer after endoscopic mucosal resection or endoscopic submucosal dissection: a meta-analysis of randomized trials. Digestion. 2011; 84:315–320.72. Zullo A, Manta R, De Francesco V, et al. Endoscopic submucosal dissection of gastric neoplastic lesions in Western countries: systematic review and meta-analysis. Eur J Gastroenterol Hepatol. 2021; 33:e1–e6.73. Ngamruengphong S, Ferri L, Aihara H, et al. Efficacy of endoscopic submucosal dissection for superficial gastric neoplasia in a large cohort in North America. Clin Gastroenterol Hepatol. 2021; 19:1611–1619.74. Libânio D, Costa MN, Pimentel-Nunes P, et al. Risk factors for bleeding after gastric endoscopic submucosal dissection: a systematic review and meta-analysis. Gastrointest Endosc. 2016; 84:572–586.75. Hatta W, Tsuji Y, Yoshio T, et al. Prediction model of bleeding after endoscopic submucosal dissection for early gastric cancer: BEST-J score. Gut. 2021; 70:476–484.76. Fujimoto K, Fujishiro M, Kato M, et al. Guidelines for gastroenterological endoscopy in patients undergoing antithrombotic treatment. Dig Endosc. 2014; 26:1–14.77. Mochizuki S, Uedo N, Oda I, et al. Scheduled second-look endoscopy is not recommended after endoscopic submucosal dissection for gastric neoplasms (the SAFE trial): a multicentre prospective randomised controlled non-inferiority trial. Gut. 2015; 64:397–405.78. Ryu HY, Kim JW, Kim HS, et al. Second-look endoscopy is not associated with better clinical outcomes after gastric endoscopic submucosal dissection: a prospective, randomized, clinical trial analyzed on an as-treated basis. Gastrointest Endosc. 2013; 78:285–294.79. Kim JS, Chung MW, Chung CY, et al. The need for second-look endoscopy to prevent delayed bleeding after endoscopic submucosal dissection for gastric neoplasms: a prospective randomized trial. Gut Liver. 2014; 8:480–486.80. Uozumi T, Sumiyoshi T, Tomita Y, et al. Does second-look endoscopy reduce the bleeding after gastric endoscopic submucosal dissection for patients receiving antithrombotic therapy? BMC Cancer. 2021; 21:946.81. Kataoka Y, Tsuji Y, Hirasawa K, et al. Endoscopic tissue shielding to prevent bleeding after endoscopic submucosal dissection: a prospective multicenter randomized controlled trial. Endoscopy. 2019; 51:619–627.82. Kawata N, Ono H, Takizawa K, et al. Efficacy of polyglycolic acid sheets and fibrin glue for prevention of bleeding after gastric endoscopic submucosal dissection in patients under continued antithrombotic agents. Gastric Cancer. 2018; 21:696–702.83. Ego M, Abe S, Nonaka S, et al. Endoscopic closure utilizing endoloop and endoclips after gastric endoscopic submucosal dissection for patients on antithrombotic therapy. Dig Dis Sci. 2021; 66:2336–2344.84. Maekawa S, Nomura R, Murase T, et al. Complete closure of artificial gastric ulcer after endoscopic submucosal dissection by combined use of a single over-the-scope clip and through-the-scope clips (with videos). Surg Endosc. 2015; 29:500–504.85. Akimoto T, Goto O, Sasaki M, et al. Endoscopic hand suturing for mucosal defect closure after gastric endoscopic submucosal dissection may reduce the risk of postoperative bleeding in patients receiving antithrombotic therapy. Dig Endosc. 2022; 34:123–132.86. Goto O, Oyama T, Ono H, et al. Endoscopic hand-suturing is feasible, safe, and may reduce bleeding risk after gastric endoscopic submucosal dissection: a multicenter pilot study (with video). Gastrointest Endosc. 2020; 91:1195–1202.87. Jung DH, Moon HS, Park CH, et al. Polysaccharide hemostatic powder to prevent bleeding after endoscopic submucosal dissection in high risk patients: a randomized controlled trial. Endoscopy. 2021; 53:994–1002.88. Hahn KY, Park JC, Lee YK, et al. Efficacy of hemostatic powder in preventing bleeding after gastric endoscopic submucosal dissection in high-risk patients. J Gastroenterol Hepatol. 2018; 33:656–663.89. Prei JC, Barmeyer C, Bürgel N, et al. EndoClot polysaccharide hemostatic system in nonvariceal gastrointestinal bleeding: results of a prospective multicenter observational pilot study. J Clin Gastroenterol. 2016; 50:e95–e100.90. Tsunada S, Ogata S, Mannen K, et al. Case series of endoscopic balloon dilation to treat a stricture caused by circumferential resection of the gastric antrum by endoscopic submucosal dissection. Gastrointest Endosc. 2008; 67:979–983.91. Coda S, Oda I, Gotoda T, et al. Risk factors for cardiac and pyloric stenosis after endoscopic submucosal dissection, and efficacy of endoscopic balloon dilation treatment. Endoscopy. 2009; 41:421–426.92. Iizuka H, Kakizaki S, Sohara N, et al. Stricture after endoscopic submucosal dissection for early gastric cancers and adenomas. Dig Endosc. 2010; 22:282–288.93. Kakushima N, Tanaka M, Sawai H, et al. Gastric obstruction after endoscopic submucosal dissection. United European Gastroenterol J. 2013; 1:184–190.94. Sumiyoshi T, Kondo H, Minagawa T, et al. Risk factors and management for gastric stenosis after endoscopic submucosal dissection for gastric epithelial neoplasm. Gastric Cancer. 2017; 20:690–698.95. Kishida Y, Kakushima N, Takizawa K, et al. Effects of steroid use for stenosis prevention after wide endoscopic submucosal dissection for gastric neoplasm. Surg Endosc. 2018; 32:751–759.96. Yoshida M, Yabuuchi Y, Kakushima N, et al. The incidence of non-ampullary duodenal cancer in Japan: the first analysis of a national cancer registry. J Gastroenterol Hepatol. 2021; 36:1216–1221.97. Goda K, Kikuchi D, Yamamoto Y, et al. Endoscopic diagnosis of superficial non-ampullary duodenal epithelial tumors in Japan: multicenter case series. Dig Endosc. 2014; 26 Suppl 2:23–29.98. Yamasaki Y, Uedo N, Akamatsu T, et al. Nonrecurrence rate of underwater EMR for ≤20-mm nonampullary duodenal adenomas: a multicenter prospective study (D-UEMR Study). Clin Gastroenterol Hepatol. 2022; 20:1010–1018.99. Kiguchi Y, Kato M, Nakayama A, et al. Feasibility study comparing underwater endoscopic mucosal resection and conventional endoscopic mucosal resection for superficial non-ampullary duodenal epithelial tumor < 20 mm. Dig Endosc. 2020; 32:753–760.100. Yamasaki Y, Uedo N, Takeuchi Y, et al. Underwater endoscopic mucosal resection for superficial nonampullary duodenal adenomas. Endoscopy. 2018; 50:154–158.101. Maruoka D, Arai M, Ishigami H, et al. Cold polypectomy for nonampullary duodenal adenoma. Endoscopy. 2015; 47 Suppl 1 UCTN:E477–E478.102. Hamada K, Takeuchi Y, Ishikawa H, et al. Safety of cold snare polypectomy for duodenal adenomas in familial adenomatous polyposis: a prospective exploratory study. Endoscopy. 2018; 50:511–517.103. Kato M, Takeuchi Y, Hoteya S, et al. Outcomes of endoscopic resection for superficial duodenal tumors: 10 years’ experience in 18 Japanese high volume centers. Endoscopy. 2022; 54:663–670.104. Kuroki K, Sanomura Y, Oka S, et al. Clinical outcomes of endoscopic resection for superficial non-ampullary duodenal tumors. Endosc Int Open. 2020; 8:E354–E359.105. Yahagi N, Kato M, Ochiai Y, et al. Outcomes of endoscopic resection for superficial duodenal epithelial neoplasia. Gastrointest Endosc. 2018; 88:676–682.106. Fukuhara S, Kato M, Iwasaki E, et al. Management of perforation related to endoscopic submucosal dissection for superficial duodenal epithelial tumors. Gastrointest Endosc. 2020; 91:1129–1137.107. Tsutsumi K, Kato M, Kakushima N, et al. Efficacy of endoscopic preventive procedures to reduce delayed adverse events after endoscopic resection of superficial nonampullary duodenal epithelial tumors: a meta-analysis of observational comparative trials. Gastrointest Endosc. 2021; 93:367–374.108. Mizutani M, Kato M, Sasaki M, et al. Predictors of technical difficulty for complete closure of mucosal defects after duodenal endoscopic resection. Gastrointest Endosc. 2021; 94:786–794.109. Yahagi N, Nishizawa T, Akimoto T, et al. New endoscopic suturing method: string clip suturing method. Gastrointest Endosc. 2016; 84:1064–1065.110. Ye LP, Mao XL, Zheng HH, et al. Safety of endoscopic resection for duodenal subepithelial lesions with wound closure using clips and an endoloop: an analysis of 68 cases. Surg Endosc. 2017; 31:1070–1077.111. Mori H, Shintaro F, Kobara H, et al. Successful closing of duodenal ulcer after endoscopic submucosal dissection with over-the-scope clip to prevent delayed perforation. Dig Endosc. 2013; 25:459–461.112. Doyama H, Tominaga K, Yoshida N, et al. Endoscopic tissue shielding with polyglycolic acid sheets, fibrin glue and clips to prevent delayed perforation after duodenal endoscopic resection. Dig Endosc. 2014; 26 Suppl 2:41–45.113. Takimoto K, Imai Y, Matsuyama K. Endoscopic tissue shielding method with polyglycolic acid sheets and fibrin glue to prevent delayed perforation after duodenal endoscopic submucosal dissection. Dig Endosc. 2014; 26 Suppl 2:46–49.114. Fukuhara S, Kato M, Iwasaki E, et al. External drainage of bile and pancreatic juice after endoscopic submucosal dissection for duodenal neoplasm: feasibility study (with video). Dig Endosc. 2021; 33:977–984.115. Abe H, Hatta W, Ogata Y, et al. Prevention of delayed bleeding with vonoprazan in upper gastrointestinal endoscopic treatment. J Gastroenterol. 2021; 56:640–650.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Endoscopic Treatment of Submucosal Tumor from Upper Gastrointestinal Tract
- Current Techniques for Treating Gastrointestinal Stromal Tumors in the Upper Gastrointestinal Tract
- Natural Orifice Transluminal Endoscopic Surgery and Upper Gastrointestinal Tract
- Endoscopic Treatment of Subepithelial Tumors
- Endoscopically resected duodenal lipoma as an uncommon cause of upper gastrointestinal bleeding: a case report
