Bolus intertransverse process block and continuous erector spinae plane block for perioperative analgesic management of video-assisted thoracoscopic surgery - Three cases report -
- Affiliations
-
- 1Department of Anesthesiology, Nara Prefecture General Medical Center, Nara, Japan
- 2Department of Anesthesiology, Nara Medical University, Nara, Japan
- KMID: 2543661
- DOI: http://doi.org/10.17085/apm.22250
Abstract
- Background
Common regional anesthesia approaches for video-assisted thoracoscopic surgery (VATS) include paravertebral block (PVB) and erector spinae plane block (ESPB). PVB is considered a deep nerve block which is contraindicated in antithrombotic therapy. ESPB is effective when administered as a bolus, as well as continuously. However, the recently proposed intertransverse process block (ITPB) ensures more effective diffusion of the local anesthetic into the paravertebral space. Case: We report cases of three patients who received bolus ITPB (costotransverse foramen block and mid-point transverse process-to-pleura block in one and two cases, respectively) combined with continuous ESPB when a deep nerve block could not be administered. Opioids were not required postoperatively, and all postoperative numerical rating scale scores (0–10) at rest were maintained below 4.
Conclusions
The combination of bolus ITPB and continuous ESPB may be an alternative analgesic method when deep nerve blocks are contraindicated in VATS.
Keyword
Figure
-
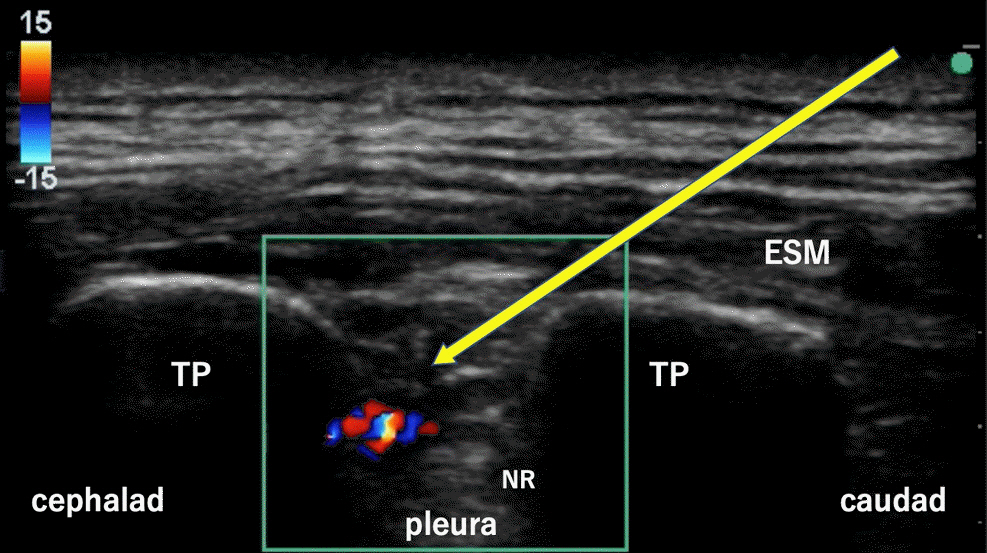
Fig. 1. Ultrasonographic visualization of a costotransverse foramen block (case 1). Color Doppler was used to confirm local anesthetic administration. ESM: erector spinae muscle, NR: neck of the rib, TP: transverse process. Yellow arrow: needle pathway.

Fig. 2. Ultrasound image after catheterization into the erector spinae plane (case 1). Normal saline solution was used to confirm the correct catheter insertion position. ESM: erector spinae muscle, NS: normal saline solution, TP: transverse process. White arrowhead: catheter.

Fig. 3. Schema representing the point of local anesthetic administration by the nerve blocks. ESPB targets the erector spinae plane, PVB targets deeper than the SCTL, and CTFB and MTPB target sites deeper than the erector spinae plane but shallower than the SCTL. These blocks allow the local anesthetic to reach the PVS more easily compared to ESPB (orange arrows). It should be noted that the puncture point and CTFB image can only be obtained by moving the probe slightly more medially. CTFB: costotransverse foramen block, ESPB: erector spinae plane block, MTPB: mid-point transverse process-to-pleura block, PVB: paravertebral block, PVS: paravertebral space, SCTL: superior costotransverse ligament, TP: transverse process.
Cited by 2 articles
-
Inter-transverse process blocks: caution about difference in methods
Raghuraman M Sethuraman
Anesth Pain Med. 2023;18(3):325-326. doi: 10.17085/apm.23050.Reply to letter to the editor: Inter-transverse process blocks: caution about difference in methods
Nobuhiro Tanaka, Yuma Kadoya, Takanori Suzuka, Masahiko Kawaguchi
Anesth Pain Med. 2024;19(1):68-69. doi: 10.17085/apm.23121.
Reference
-
1. Bendixen M, Jørgensen OD, Kronborg C, Andersen C, Licht PB. Postoperative pain and quality of life after lobectomy via video-assisted thoracoscopic surgery or anterolateral thoracotomy for early stage lung cancer: a randomised controlled trial. Lancet Oncol. 2016; 17:836–44.
Article2. Batchelor TJP, Rasburn NJ, Abdelnour-Berchtold E, Brunelli A, Cerfolio RJ, Gonzalez M, et al. Guidelines for enhanced recovery after lung surgery: recommendations of the Enhanced Recovery After Surgery (ERAS®) Society and the European Society of Thoracic Surgeons (ESTS). Eur J Cardiothorac Surg. 2019; 55:91–115.
Article3. Feray S, Lubach J, Joshi GP, Bonnet F, Van de Velde M; PROSPECT Working Group *of the European Society of Regional Anaesthesia and Pain Therapy. PROSPECT guidelines for video-assisted thoracoscopic surgery: a systematic review and procedure-specific postoperative pain management recommendations. Anaesthesia. 2022; 77:311–25.
Article4. Taketa Y, Irisawa Y, Fujitani T. Comparison of ultrasound-guided erector spinae plane block and thoracic paravertebral block for postoperative analgesia after video-assisted thoracic surgery: a randomized controlled non-inferiority clinical trial. Reg Anesth Pain Med. 2020; 45:10–5.
Article5. Kim SH. Anatomical classification and clinical application of thoracic paraspinal blocks. Korean J Anesthesiol. 2022; 75:295–306.
Article6. Costache I, de Neumann L, Ramnanan CJ, Goodwin SL, Pawa A, Abdallah FW, et al. The mid-point transverse process to pleura (MTP) block: a new end-point for thoracic paravertebral block. Anaesthesia. 2017; 72:1230–6.
Article7. Shibata Y, Kampitak W, Tansatit T. The novel costotransverse foramen block technique: distribution characteristics of injectate compared with erector spinae plane block. Pain Physician. 2020; 23:E305–14.8. El-Boghdadly K, Wolmarans M, Stengel AD, Albrecht E, Chin KJ, Elsharkawy H, et al. Standardizing nomenclature in regional anesthesia: an ASRA-ESRA Delphi consensus study of abdominal wall, paraspinal, and chest wall blocks. Reg Anesth Pain Med. 2021; 46:571–80.
Article9. Swathi KB, Kamal M, Kumar M, Kumar R, Chhabra S, Bhatia P. Comparison of analgesic efficacy of the conventional approach and mid-transverse process to pleura approach of the paravertebral block in video-assisted thoracoscopy surgeries: a randomised controlled trial. Indian J Anaesth. 2021; 65:512–8.
Article10. Kietaibl S, Ferrandis R, Godier A, Llau J, Lobo C, Macfarlane AJ, et al. Regional anaesthesia in patients on antithrombotic drugs: joint ESAIC/ESRA guidelines. Eur J Anaesthesiol. 2022; 39:100–32.11. Davies RG, Myles PS, Graham JM. A comparison of the analgesic efficacy and side-effects of paravertebral vs epidural blockade for thoracotomy--a systematic review and meta-analysis of randomized trials. Br J Anaesth 2006; 96: 418-26. Erratum in: Br J Anaesth. 2007; 99:768.12. Chen X, Yang J, Xia M, Wu H, Wang S, Zhang W. Single-injection midpoint transverse process-to- pleura block versus thoracic paravertebral block for postoperative analgesia after uniportal video-assisted thoracoscopic surgery: a randomized controlled trial. J Cardiothorac Vasc Anesth. 2022; 36(8 Pt A):2432–8.
Article13. Chin KJ, El-Boghdadly K. Mechanisms of action of the erector spinae plane (ESP) block: a narrative review. Can J Anaesth. 2021; 68:387–408.
Article14. Cho TH, Kim SH, O J, Kwon HJ, Kim KW, Yang HM. Anatomy of the thoracic paravertebral space: 3D micro-CT findings and their clinical implications for nerve blockade. Reg Anesth Pain Med. 2021; 46:699–703.
Article15. Tsui BCH, Fonseca A, Munshey F, McFadyen G, Caruso TJ. The erector spinae plane (ESP) block: a pooled review of 242 cases. J Clin Anesth. 2019; 53:29–34.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Anatomical classification and clinical application of thoracic paraspinal blocks
- Erector spinae plane block for spinal surgery: a systematic review and meta-analysis
- Erector spinae plane block for pediatric hip surgery: a case report
- Magnetic Resonance Imaging Images of the Local Anesthetic Spreading after Erector Spinae Plane Block at T2 Level
- Analgesic Effect of Erector Spinae Plane Block at T2 Level in Arm Surgery
