Targeted temperature management in a patient with suspected hypoxic-ischemic brain injury after successful resuscitation from cardiac arrest: a case report
- Affiliations
-
- 1Department of Anesthesia and Pain Medicine, Seoul National University Hospital, Seoul, Korea
- 2Department of Anesthesia and Pain Medicine and Biomedical Research Institute, Pusan National University Hospital, Pusan, Korea
- 3Department of Anesthesia and Pain Medicine, Pusan National University School of Medicine, Busan, Korea
- KMID: 2543335
- DOI: http://doi.org/10.7180/kmj.22.130
Abstract
- Hypoxic-ischemic brain injury (HIBI) after cardiac arrest (CA) is a leading cause of mortality and long-term neurological disorders in survivors. Targeted temperature management (TTM) has been rigorously studied as a way to improve results compared to a normal body temperature for preventing secondary damage after HIBI. We report a case of successful TTM in a patient who was suspected to have HIBI after resuscitation from cardiovascular collapse due to respiratory failure during elective surgery under brachial plexus block with dexmedetomidine and remifentanil infusion. A 27-year-old male patient developed CA due to apnea during orthopedic surgery. TTM was performed in the surgical intensive care unit for 72 hours after resuscitation, and the patient recovered successfully. TTM application immediately after resuscitation from CA in patients with suspected HIBI may be an appropriate treatment.
Keyword
Figure
-

Fig. 1. Timeline of cardiopulmonary resuscitation and patient treatment with changes in vital signs, ABGA, electrolytes, glucose, and lactic acid. MRI, magnetic resonance imaging; SCIU, surgical intensive care unit; TTM, targeted temperature management; CPCR, cardiopulmonary cerebral resuscitation; BPB, brachial plexus block; DMT, dexmedetomidine; IV, intravenous; BIS, bispectral index; ABGA, arterial blood gas analysis; ER, emergency room; BP, blood pressure; ROSC, return of spontaneous circulation; b-MRI, brain MRI; BT, body temperature; HR, heart rate; SpO2, saturation by pulse oximetry; Hb, hemoglobin; PaCO2, arterial carbon dioxide pressure; O2 Sat, SaO2 saturation of arterial oxygen; PaO2, arterial oxygen pressure; Hct, hematocrit.
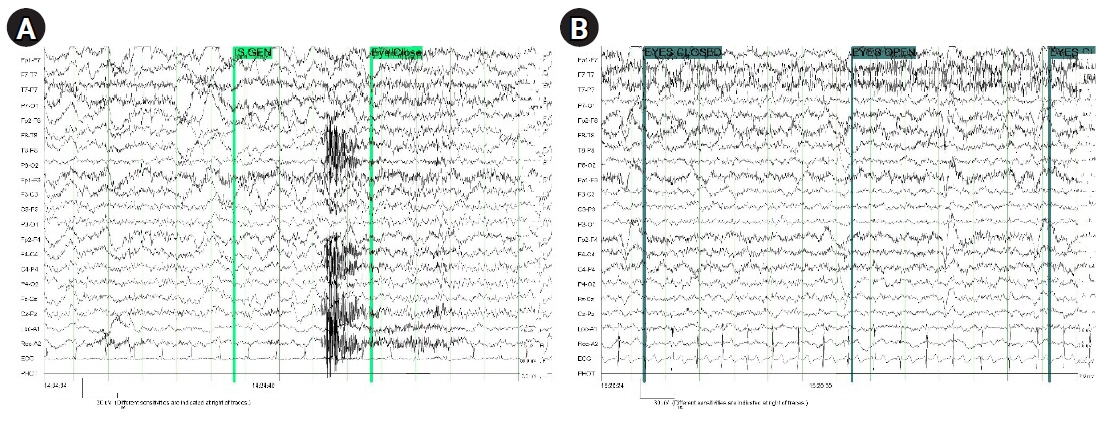
Fig. 2. Electroencephalography findings were suggestive of mild diffuse cerebral dysfunction. (A) During target temperature management. (B) After regaining of consciousness.
Reference
-
References
1. Sekhon MS, Ainslie PN, Griesdale DE. Clinical pathophysiology of hypoxic ischemic brain injury after cardiac arrest: a “two-hit” model. Crit Care. 2017; 21:90.2. Nielsen N, Wetterslev J, Cronberg T, Erlinge D, Gasche Y, Hassager C, et al. Targeted temperature management at 33°C versus 36°C after cardiac arrest. N Engl J Med. 2013; 369:2197–206.3. Weerink MA, Barends CR, Muskiet ER, Reyntjens KM, Knotnerus FH, Oostra M, et al. Pharmacodynamic interaction of remifentanil and dexmedetomidine on depth of sedation and tolerance of laryngoscopy. Anesthesiology. 2019; 131:1004–17.4. Bloor BC, Ward DS, Belleville JP, Maze M. Effects of intravenous dexmedetomidine in humans. II. Hemodynamic changes. Anesthesiology. 1992; 77:1134–42.5. Makita K, Ishikawa S. Remifentanil. Masui. 2006; 55:817–25.6. Feng G, Jiang G, Li Z, Wang X. Prognostic value of electroencephalography (EEG) for brain injury after cardiopulmonary resuscitation. Neurol Sci. 2016; 37:843–9.7. Goodman PG, Mehta AR, Castresana MR. Predicting ischemic brain injury after intraoperative cardiac arrest during cardiac surgery using the BIS monitor. J Clin Anesth. 2009; 21:609–12.8. Sandroni C, D’Arrigo S, Nolan JP. Prognostication after cardiac arrest. Crit Care. 2018; 22:150.9. Endisch C, Storm C, Ploner CJ, Leithner C. Amplitudes of SSEP and outcome in cardiac arrest survivors: a prospective cohort study. Neurology. 2015; 85:1752–60.10. Chen Z, Ding Y, Ji X, Meng R. Advances in normobaric hyperoxia brain protection in experimental stroke. Front Neurol. 2020; 11:50.11. Walker AC, Johnson NJ. Targeted temperature management and postcardiac arrest care. Emerg Med Clin North Am. 2019; 37:381–93.12. Kuisma M, Boyd J, Voipio V, Alaspaa A, Roine RO, Rosenberg P. Comparison of 30 and the 100% inspired oxygen concentrations during early post-resuscitation period: a randomised controlled pilot study. Resuscitation. 2006; 69:199–206.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Targeted temperature management with hypothermia for comatose patients after cardiac arrest
- Prolonged Delirium Secondary to Hypoxic-ischemic Encephalopathy Following Cardiac Arrest
- Clinical Implementation of Therapeutic Hypothermia after Cardiac Arrest
- A Case Report of Spinal Cord Ischemia after Cardiopulmonary Resuscitation
- Management of Brain Injury after Post-cardiac Arrest Syndrome
