Impact of Pulmonary Arterial Elastance on Right Ventricular Mechanics and Exercise Capacity in Repaired Tetralogy of Fallot
- Affiliations
-
- 1Department of Pediatrics, Sejong General Hospital, Bucheon, Korea
- 2The Sixth Affiliated Hospital of Harbin Medical University, Harbin, China
- 3Department of Thoracic and Cardiovascular Surgery, Sejong General Hospital, Bucheon, Korea
- KMID: 2543053
- DOI: http://doi.org/10.4070/kcj.2022.0228
Abstract
- Background and Objectives
Pathophysiological changes of right ventricle (RV) after repair of tetralogy of Fallot (TOF) are coupled with a highly compliant low-pressure pulmonary artery (PA) system. This study aimed to determine whether pulmonary vascular function was associated with RV parameters and exercise capacity, and its impact on RV remodeling after pulmonary valve replacement.
Methods
In a total of 48 patients over 18 years of age with repaired TOF, pulmonary arterial elastance (Ea), RV volume data, and RV-PA coupling ratio were calculated and analyzed in relation to exercise capacity.
Results
Patients with a low Ea showed a more severe pulmonary regurgitation volume index, greater RV end-diastolic volume index, and greater effective RV stroke volume (p=0.039, p=0.013, and p=0.011, respectively). Patients with a high Ea had lower exercise capacity than those with a low Ea (peak oxygen consumption [peak VO2 ] rate: 25.8±7.7 vs. 34.3±5.5 mL/kg/min, respectively, p=0.003), while peak VO2 was inversely correlated with Ea and mean PA pressure (p=0.004 and p=0.004, respectively). In the univariate analysis, a higher preoperative RV end-diastolic volume index and RV end-systolic volume index, left ventricular end-systolic volume index, and higher RV-PA coupling ratio were risk factors for suboptimal outcomes. Preoperative RV volume and RV-PA coupling ratio reflecting the adaptive PA system response are important factors in optimal postoperative results.
Conclusions
We found that PA vascular dysfunction, presenting as elevated Ea in TOF, may contribute to exercise intolerance. However, Ea was inversely correlated with pulmonary regurgitation (PR) severity, which may prevent PR, RV dilatation, and left ventricular dilatation in the absence of significant pulmonary stenosis.
Keyword
Figure
-
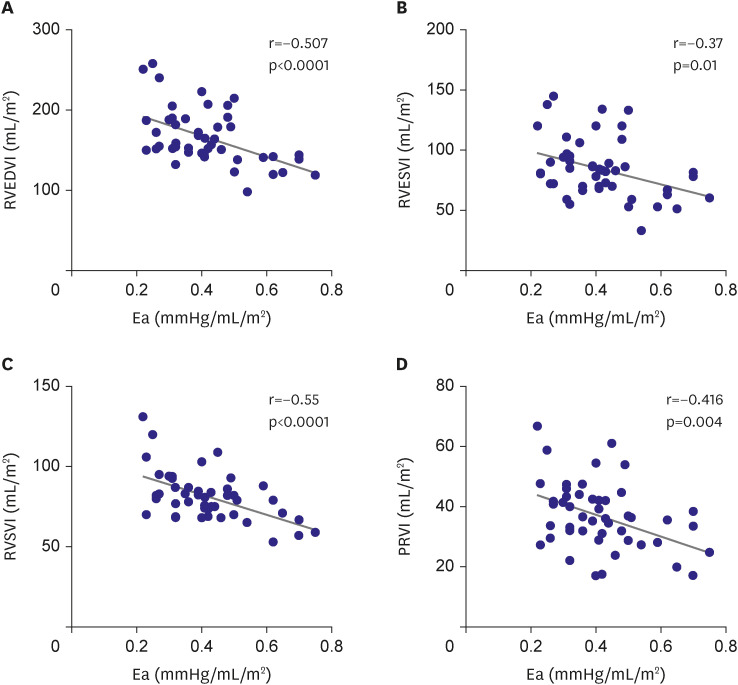
Figure 1 Correlation between pulmonary Ea and right ventricular volumetric indices. The Ea is negatively correlated with PRVi (r=−0.416, p=004), RVEDVi (r=−0.507, p<0.0001), RVESVi (r=−0.37, p=0.01), and RVSVi (r=−0.55, p<0.0001).Ea = arterial elastance; PRVi = pulmonary regurgitant volume index; RVEDVi = right ventricular end-diastolic volume index; RVESVi = right ventricular end-systolic volume index; RVSVi = right ventricular stroke volume index.
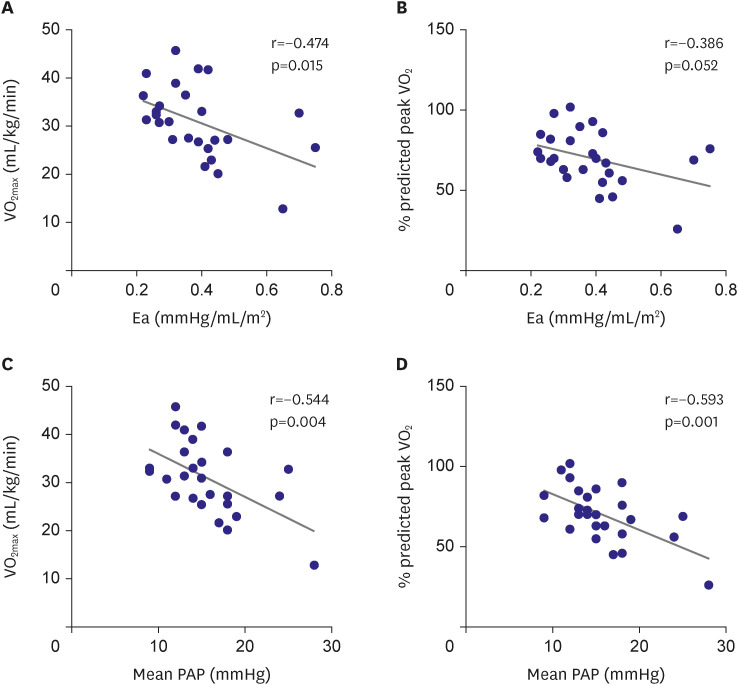
Figure 2 Correlation between exercise capacity and several variables. (A) Pulmonary Ea had a negative correlation with VO2max (r=−0.474, p=0.015). (B) Ea did not have significant correlation with % predicted peak VO2 (r=−0.386, p=0.052). (C) Mean PAP exhibit a negative correlation with VO2max (r=−0.544, p=0.004) and (D) % predicted peak VO2 (r=−0.593, p=0.001).Ea = arterial elastance; PAP =pulmonary artery pressure; peak VO2 = peak oxygen consumption; VO2max = maximal oxygen consumption.
Reference
-
1. Gatzoulis MA, Balaji S, Webber SA, et al. Risk factors for arrhythmia and sudden cardiac death late after repair of tetralogy of Fallot: a multicentre study. Lancet. 2000; 356:975–981. PMID: 11041398.2. Geva T, Sandweiss BM, Gauvreau K, Lock JE, Powell AJ. Factors associated with impaired clinical status in long-term survivors of tetralogy of Fallot repair evaluated by magnetic resonance imaging. J Am Coll Cardiol. 2004; 43:1068–1074. PMID: 15028368.3. Oosterhof T, van Straten A, Vliegen HW, et al. Preoperative thresholds for pulmonary valve replacement in patients with corrected tetralogy of Fallot using cardiovascular magnetic resonance. Circulation. 2007; 116:545–551. PMID: 17620511.4. Dave HH, Buechel ER, Dodge-Khatami A, et al. Early insertion of a pulmonary valve for chronic regurgitation helps restoration of ventricular dimensions. Ann Thorac Surg. 2005; 80:1615–1620. PMID: 16242426.5. Geva T, Mulder B, Gauvreau K, et al. Preoperative predictors of death and sustained ventricular tachycardia after pulmonary valve replacement in patients with repaired tetralogy of Fallot enrolled in the INDICATOR cohort. Circulation. 2018; 138:2106–2115. PMID: 30030416.6. Bédard E, McCarthy KP, Dimopoulos K, Giannakoulas G, Gatzoulis MA, Ho SY. Structural abnormalities of the pulmonary trunk in tetralogy of Fallot and potential clinical implications: a morphological study. J Am Coll Cardiol. 2009; 54:1883–1890. PMID: 19892240.7. Kilner PJ, Balossino R, Dubini G, et al. Pulmonary regurgitation: the effects of varying pulmonary artery compliance, and of increased resistance proximal or distal to the compliance. Int J Cardiol. 2009; 133:157–166. PMID: 18722025.8. Gatzoulis MA, Till JA, Somerville J, Redington AN. Mechanoelectrical interaction in tetralogy of Fallot. QRS prolongation relates to right ventricular size and predicts malignant ventricular arrhythmias and sudden death. Circulation. 1995; 92:231–237. PMID: 7600655.9. Egbe AC, Kothapalli S, Miranda WR, et al. Assessment of right ventricular-pulmonary arterial coupling in chronic pulmonary regurgitation. Can J Cardiol. 2019; 35:914–922. PMID: 31292091.10. Lee C, Kim YM, Lee CH, et al. Outcomes of pulmonary valve replacement in 170 patients with chronic pulmonary regurgitation after relief of right ventricular outflow tract obstruction: implications for optimal timing of pulmonary valve replacement. J Am Coll Cardiol. 2012; 60:1005–1014. PMID: 22921969.11. Rominger MB, Bachmann GF, Pabst W, Rau WS. Right ventricular volumes and ejection fraction with fast cine MR imaging in breath-hold technique: applicability, normal values from 52 volunteers, and evaluation of 325 adult cardiac patients. J Magn Reson Imaging. 1999; 10:908–918. PMID: 10581503.12. Trip P, Kind T, van de Veerdonk MC, et al. Accurate assessment of load-independent right ventricular systolic function in patients with pulmonary hypertension. J Heart Lung Transplant. 2013; 32:50–55. PMID: 23164535.13. Oosterhof T, Mulder BJ, Vliegen HW, de Roos A. Cardiovascular magnetic resonance in the follow-up of patients with corrected tetralogy of Fallot: a review. Am Heart J. 2006; 151:265–272. PMID: 16442887.14. Inuzuka R, Seki M, Sugimoto M, Saiki H, Masutani S, Senzaki H. Pulmonary arterial wall stiffness and its impact on right ventricular afterload in patients with repaired tetralogy of Fallot. Ann Thorac Surg. 2013; 96:1435–1441. PMID: 23972390.15. Egbe AC, Anavekar NS, Connolly HM. Abnormal pulmonary arterial elastance is associated with reduced exercise capacity in tetralogy of Fallot. J Am Heart Assoc. 2019; 8:e011731. PMID: 31181980.16. Gorter TM, Obokata M, Reddy YN, Melenovsky V, Borlaug BA. Exercise unmasks distinct pathophysiologic features in heart failure with preserved ejection fraction and pulmonary vascular disease. Eur Heart J. 2018; 39:2825–2835. PMID: 29947750.17. Borlaug BA, Kane GC, Melenovsky V, Olson TP. Abnormal right ventricular-pulmonary artery coupling with exercise in heart failure with preserved ejection fraction. Eur Heart J. 2016; 37:3293–3302.18. Melenovsky V, Hwang SJ, Lin G, Redfield MM, Borlaug BA. Right heart dysfunction in heart failure with preserved ejection fraction. Eur Heart J. 2014; 35:3452–3462. PMID: 24875795.19. Yap J, Tan JL, Le TT, et al. Assessment of left ventricular preload by cardiac magnetic resonance imaging predicts exercise capacity in adult operated tetralogy of Fallot: a retrospective study. BMC Cardiovasc Disord. 2014; 14:122. PMID: 25245139.20. Gnanappa GK, Celermajer DS, Zhu D, Puranik R, Ayer J. Severe right ventricular dilatation after repair of Tetralogy of Fallot is associated with increased left ventricular preload and stroke volume. Eur Heart J Cardiovasc Imaging. 2019; 20:1020–1026. PMID: 30874802.21. O’Meagher S, Munoz PA, Alison JA, et al. Exercise capacity and stroke volume are preserved late after tetralogy repair, despite severe right ventricular dilatation. Heart. 2012; 98:1595–1599. PMID: 22869677.22. Meadows J, Powell AJ, Geva T, Dorfman A, Gauvreau K, Rhodes J. Cardiac magnetic resonance imaging correlates of exercise capacity in patients with surgically repaired tetralogy of Fallot. Am J Cardiol. 2007; 100:1446–1450. PMID: 17950806.23. Latus H, Binder W, Kerst G, Hofbeck M, Sieverding L, Apitz C. Right ventricular-pulmonary arterial coupling in patients after repair of tetralogy of Fallot. J Thorac Cardiovasc Surg. 2013; 146:1366–1372. PMID: 23507126.24. Maughan WL, Sunagawa K, Sagawa K. Effects of arterial input impedance on mean ventricular pressure-flow relation. Am J Physiol. 1984; 247:H978–H983. PMID: 6507645.25. Kuehne T, Yilmaz S, Steendijk P, et al. Magnetic resonance imaging analysis of right ventricular pressure-volume loops: in vivo validation and clinical application in patients with pulmonary hypertension. Circulation. 2004; 110:2010–2016. PMID: 15451801.26. Sanz J, García-Alvarez A, Fernández-Friera L, et al. Right ventriculo-arterial coupling in pulmonary hypertension: a magnetic resonance study. Heart. 2012; 98:238–243. PMID: 21917658.27. Vonk-Noordegraaf A, Haddad F, Chin KM, et al. Right heart adaptation to pulmonary arterial hypertension: physiology and pathobiology. J Am Coll Cardiol. 2013; 62:D22–D33. PMID: 24355638.28. Naeije R, Manes A. The right ventricle in pulmonary arterial hypertension. Eur Respir Rev. 2014; 23:476–487. PMID: 25445946.29. Vonk Noordegraaf A, Westerhof BE, Westerhof N. The relationship between the right ventricle and its load in pulmonary hypertension. J Am Coll Cardiol. 2017; 69:236–243. PMID: 28081831.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Rare Case of Tetralogy of Fallot Associated with Pulmonary Artery Sling
- Exercise tolerance tests in patients with tetralogy of Fallot repaired earlier: correlation with 2-dimensional echocardiography and cardiac catheterization
- Pulmonary Arterial Elastance and Right Ventricle-Pulmonary Artery Coupling in Postoperative Tetralogy of Fallot Patients
- Anesthesia for Tetralogy of Fallot - Pathophysiological view
- Tentative Results of Balloon Dilatation of the Pulmonary Valves
