Cancer Res Treat.
2023 Apr;55(2):479-487. 10.4143/crt.2022.1344.
The Role of Brain Radiotherapy before First-Line Afatinib Therapy, Compared to Gefitinib or Erlotinib, in Patients with EGFR-Mutant Non–Small Cell Lung Cancer
- Affiliations
-
- 1Division of Hematology-Oncology, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
- KMID: 2541234
- DOI: http://doi.org/10.4143/crt.2022.1344
Abstract
- Purpose
Brain metastasis is common in patients with epidermal growth factor receptor (EGFR)–mutant non–small cell lung cancer (NSCLC) at initial presentation. A previous study showed that brain radiotherapy (RT) before first-generation (first-G) EGFR–tyrosine kinase inhibitor (TKI) therapy is associated with longer overall survival than TKI therapy alone. However, there is no data regarding the role of additional brain RT before afatinib therapy.
Materials and Methods
Between October 2014 and June 2019, EGFR-mutant NSCLC patients with brain metastases who started first-G EGFR-TKIs (gefitinib or erlotinib) or afatinib as first-line therapy were retrospectively analyzed. This study compared overall survival and intracranial progression-free survival (PFS) between patients who received EGFR-TKIs alone and EGFR-TKIs with brain RT and either a first-G EGFR-TKI or afatinib, respectively.
Results
The median follow-up duration was 29.6 months (range, 1.5 to 116.9 months). In the first-G EGFR-TKI group (n=155), 94 patients (60.6%) received the first-G EGFR-TKI alone and 61 patients (39.4%) received brain RT prior to their first-G EGFR-TKI. In the afatinib group (n=204), 126 patients (61.8%) received afatinib alone and 78 patients (38.2%) received brain RT prior to afatinib. There was no difference in overall survival rates between the groups with RT (35.6 months: 95% confidence interval [CI], 27.9 to 43.3) and without RT (31.4 months: 95% CI, 23.9 to 38.9) in the afatinib group (p=0.58), but there was a significant difference in overall survival in the first-G EGFR-TKI group in a manner favoring additional brain RT (41.1 months: 95% CI, 30.5 to 51.7 vs. 25.8 months: 95% CI, 20.1 to 31.5; p=0.02). Meanwhile, median intracranial PFS was not different between patients who received EGFR-TKI therapy alone vs. EGFR-TKI therapy with brain RT in both the first-G EGFR-TKI (p=0.39) and afatinib (p=0.24) groups.
Conclusion
Afatinib therapy alone showed comparable survival outcomes to those of afatinib with brain RT. The current study suggests that brain RT could be an optional, not mandatory, treatment modality when afatinib therapy is considered in patients with EGFR-mutant NSCLC.
Figure
-
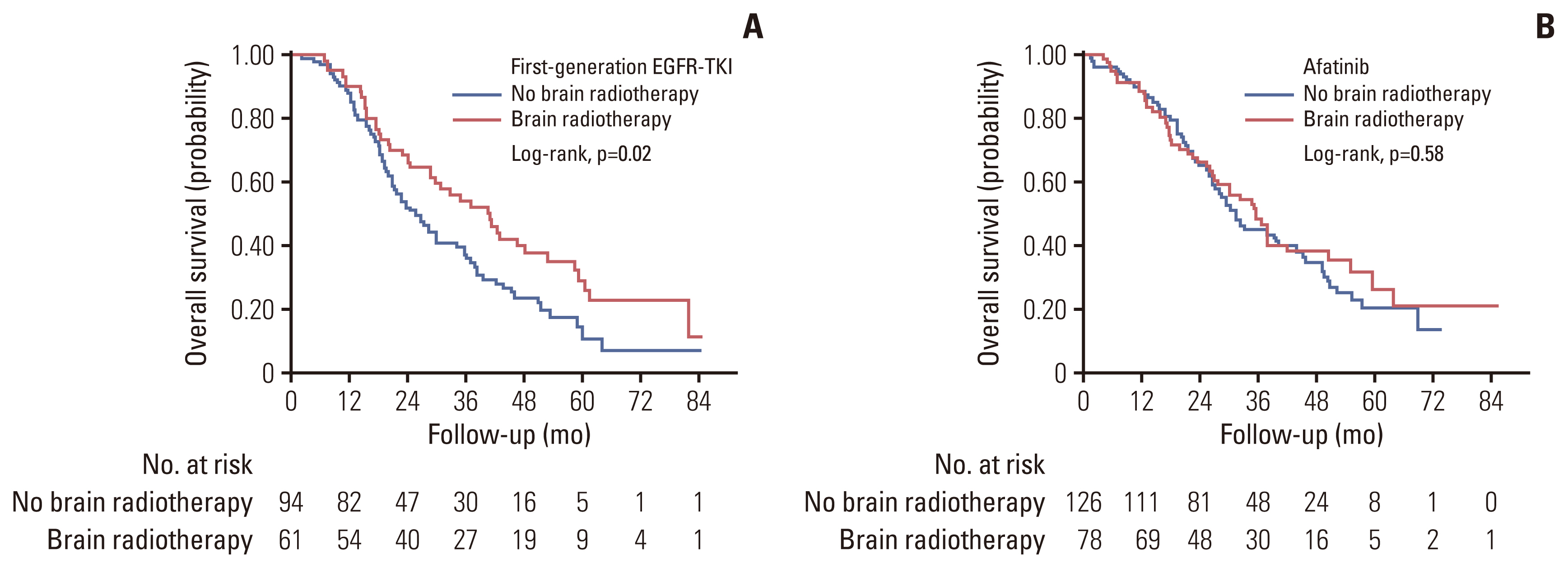
Fig. 1 Overall survival of patients with and without brain radiotherapy in the groups of first-generation epidermal growth factor receptor-tyrosine kinase inhibitor (EGFR-TKI) (A) and afatinib (B) groups.
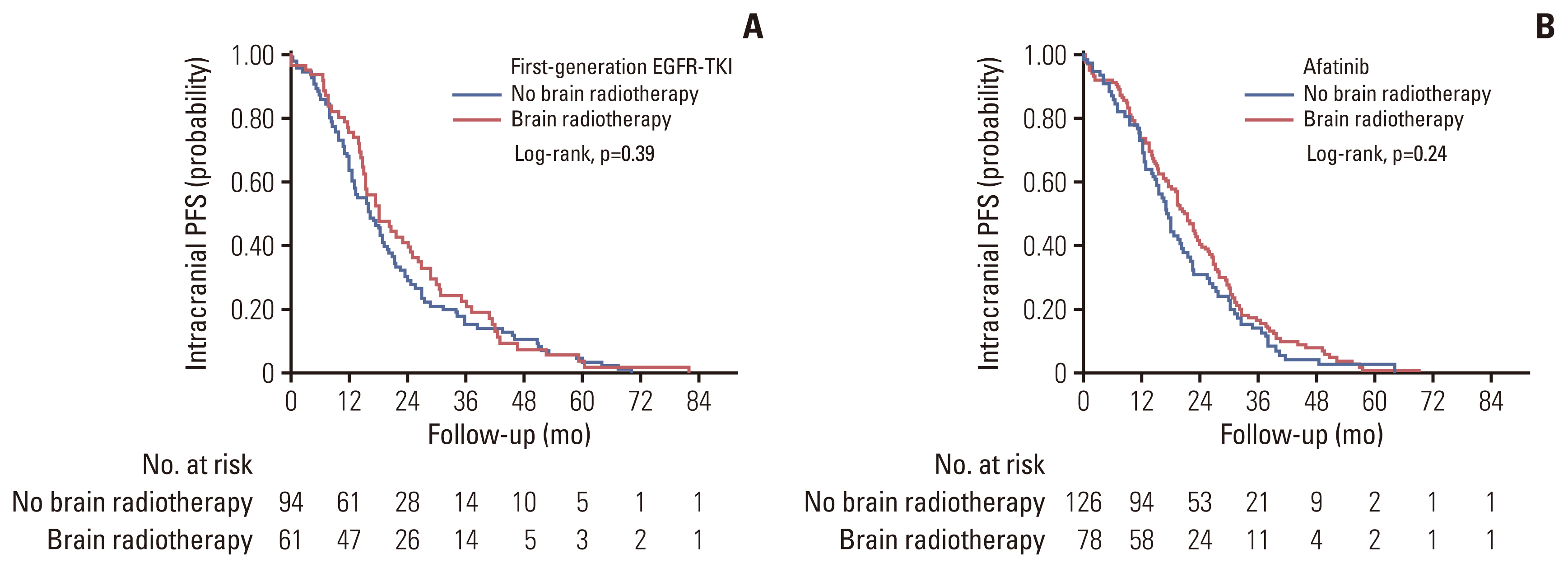
Fig. 2 Intracranial progression-free survival (PFS) of patients with and without brain radiotherapy in the groups of first-generation epidermal growth factor receptor-tyrosine kinase inhibitor (EGFR-TKI) (A) and afatinib (B) groups.
Reference
-
References
1. Sperduto PW, Kased N, Roberge D, Xu Z, Shanley R, Luo X, et al. Summary report on the graded prognostic assessment: an accurate and facile diagnosis-specific tool to estimate survival for patients with brain metastases. J Clin Oncol. 2012; 30:419–25.
Article2. Ge M, Zhuang Y, Zhou X, Huang R, Liang X, Zhan Q. High probability and frequency of EGFR mutations in non-small cell lung cancer with brain metastases. J Neurooncol. 2017; 135:413–8.
Article3. Iuchi T, Shingyoji M, Itakura M, Yokoi S, Moriya Y, Tamura H, et al. Frequency of brain metastases in non-small-cell lung cancer, and their association with epidermal growth factor receptor mutations. Int J Clin Oncol. 2015; 20:674–9.
Article4. Jung HA, Woo SY, Lee SH, Ahn JS, Ahn MJ, Park K, et al. The different central nervous system efficacy among gefitinib, erlotinib and afatinib in patients with epidermal growth factor receptor mutation-positive non-small cell lung cancer. Transl Lung Cancer Res. 2020; 9:1749–58.
Article5. Lee SY, Choi CM, Chang YS, Lee KY, Kim SJ, Yang SH, et al. Real-world experience of afatinib as first-line therapy for advanced EGFR mutation-positive non-small cell lung cancer in Korea. Transl Lung Cancer Res. 2021; 10:4353–67.
Article6. Park SJ, Kim HT, Lee DH, Kim KP, Kim SW, Suh C, et al. Efficacy of epidermal growth factor receptor tyrosine kinase inhibitors for brain metastasis in non-small cell lung cancer patients harboring either exon 19 or 21 mutation. Lung Cancer. 2012; 77:556–60.
Article7. Wei YF, Lim CK, Tsai MS, Huang MS, Chen KY. Intracranial responses to afatinib at different doses in patients with EGFR-mutated non-small-cell lung carcinoma and brain metastases. Clin Lung Cancer. 2019; 20:e274–83.
Article8. Reungwetwattana T, Nakagawa K, Cho BC, Cobo M, Cho EK, Bertolini A, et al. CNS response to osimertinib versus standard epidermal growth factor receptor tyrosine kinase inhibitors in patients with untreated EGFR-mutated advanced non-small-cell lung cancer. J Clin Oncol. 2018; 36:JCO2018783118.9. Magnuson WJ, Lester-Coll NH, Wu AJ, Yang TJ, Lockney NA, Gerber NK, et al. Management of brain metastases in tyrosine kinase inhibitor-naive epidermal growth factor receptor-mutant non-small-cell lung cancer: a retrospective multi-institutional analysis. J Clin Oncol. 2017; 35:1070–7.10. Thomas NJ, Myall NJ, Sun F, Patil T, Mushtaq R, Yu C, et al. Brain metastases in EGFR- and ALK-positive NSCLC: outcomes of central nervous system-penetrant tyrosine kinase inhibitors alone versus in combination with radiation. J Thorac Oncol. 2022; 17:116–29.
Article11. Hoffknecht P, Tufman A, Wehler T, Pelzer T, Wiewrodt R, Schutz M, et al. Efficacy of the irreversible ErbB family blocker afatinib in epidermal growth factor receptor (EGFR) tyrosine kinase inhibitor (TKI)-pretreated non-small-cell lung cancer patients with brain metastases or leptomeningeal disease. J Thorac Oncol. 2015; 10:156–63.
Article12. Kim M, Laramy JK, Mohammad AS, Talele S, Fisher J, Sarkaria JN, et al. Brain distribution of a panel of epidermal growth factor receptor inhibitors using cassette dosing in wild-type and Abcb1/Abcg2-deficient mice. Drug Metab Dispos. 2019; 47:393–404.
Article13. Li D, Ambrogio L, Shimamura T, Kubo S, Takahashi M, Chirieac LR, et al. BIBW2992, an irreversible EGFR/HER2 inhibitor highly effective in preclinical lung cancer models. Oncogene. 2008; 27:4702–11.
Article14. Brown PD, Jaeckle K, Ballman KV, Farace E, Cerhan JH, Anderson SK, et al. Effect of radiosurgery alone vs radiosurgery with whole brain radiation therapy on cognitive function in patients with 1 to 3 brain metastases: a randomized clinical trial. JAMA. 2016; 316:401–9.
Article15. Li J, Ludmir EB, Wang Y, Guha-Thakurta N, McAleer MF, Settle SH, et al. Stereotactic radiosurgery versus whole-brain radiation therapy for patients with 4–15 brain metastases: a phase III randomized controlled trial. Int J Radiat Oncol Biol Phys. 2020; 108:S21–2.
Article16. Chao ST, Ahluwalia MS, Barnett GH, Stevens GH, Murphy ES, Stockham AL, et al. Challenges with the diagnosis and treatment of cerebral radiation necrosis. Int J Radiat Oncol Biol Phys. 2013; 87:449–57.
Article17. Cho BC, Han JY, Kim SW, Lee KH, Cho EK, Lee YG, et al. A phase 1/2 study of lazertinib 240 mg in patients with advanced EGFR T790M-positive NSCLC after previous EGFR tyrosine kinase inhibitors. J Thorac Oncol. 2022; 17:558–67.
Article18. Yang JJ, Zhou C, Huang Y, Feng J, Lu S, Song Y, et al. Icotinib versus whole-brain irradiation in patients with EGFR-mutant non-small-cell lung cancer and multiple brain metastases (BRAIN): a multicentre, phase 3, open-label, parallel, randomised controlled trial. Lancet Respir Med. 2017; 5:707–16.19. Vogelbaum MA, Brown PD, Messersmith H, Brastianos PK, Burri S, Cahill D, et al. Treatment for brain metastases: ASCO-SNO-ASTRO guideline. J Clin Oncol. 2022; 40:492–516.
Article20. Yamamoto M, Serizawa T, Shuto T, Akabane A, Higuchi Y, Kawagishi J, et al. Stereotactic radiosurgery for patients with multiple brain metastases (JLGK0901): a multi-institutional prospective observational study. Lancet Oncol. 2014; 15:387–95.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Efficacy and Safety of Afatinib for EGFR-mutant Non-small Cell Lung Cancer, Compared with Gefitinib or Erlotinib
- The Clinical Outcomes of Different First-Line EGFR-TKIs Plus Bevacizumab in Advanced EGFR-Mutant Lung Adenocarcinoma
- Efficacy of epidermal growth factor receptor-tyrosine kinase inhibitors for patient with leptomeningeal metastasis of epidermal growth factor receptor mutant non-small cell lung cancer
- Comparison of the therapeutic outcome between gefitinib and erlotinib in female patients with non-small-cell lung cancer
- Successful Rechallenge with Gefitinib for an Initial Erlotinib-Responder with Advanced Lung Adenocarcinoma
