J Neurocrit Care.
2022 Dec;15(2):113-121. 10.18700/jnc.220068.
Association of chloride-rich fluids and medication diluents on the incidence of hyperchloremia and clinical consequences in aneurysmal subarachnoid hemorrhage
- Affiliations
-
- 1Memorial Hermann The Woodlands Medical Center, The Woodlands, TX, USA
- 2University of Kentucky Healthcare Chandler Medical Center, Lexington, KY, USA
- 3Kentucky Children’s Hospital, Lexington, KY, USA
- KMID: 2538768
- DOI: http://doi.org/10.18700/jnc.220068
Abstract
- Background
Chloride-rich fluid administration is frequently employed in the management of aneurysmal subarachnoid hemorrhage (aSAH). However, the incidence and consequences of hyperchloremia in aSAH remain poorly defined. This study aimed to describe the incidence of hyperchloremia in aSAH, the contribution of fluid sources to chloride exposure, and the potential associations of hyperchloremia with patient outcomes.
Methods
This was a single-center retrospective cohort study of patients admitted to a neurointensive care unit with aSAH. The primary outcome was incidence of hyperchloremia (chloride >109 mEq/L). Secondary outcomes included incidence of severe hyperchloremia (chloride >115 mEq/L), incidence of acute kidney injury (AKI), need for renal replacement therapy (RRT), intensive care unit (ICU) length of stay (LOS), hospital LOS, and in-hospital mortality.
Results
Of the 234 patients included in the analysis, hyperchloremia occurred in 75% (n=175), and 58% (n=101) developed severe hyperchloremia. Median time to onset was 3 days (interquartile range, 1–5) after admission. Hyperchloremia was associated with prolonged ICU LOS (12 vs. 8 days, P<0.001), duration of mechanical ventilation (16 vs. 10 days, P<0.001), hospital LOS (15 vs. 9 days, P<0.001), and in-hospital mortality (14.3% vs. 0%, P=0.002) compared to no hyperchloremia. No significant difference was observed in the incidence of AKI or the need for RRT. Maintenance intravenous fluids accounted for the highest proportion of the cumulative chloride burden.
Conclusion
Hyperchloremia occurs at a high frequency in aSAH and is associated with poor patient outcomes. Maintenance intravenous fluids accounted for the highest proportion of cumulative chloride burden.
Figure
-

Fig. 1. Median daily serum chloride trend over the 14-day study period. AKI, acute kidney injury.
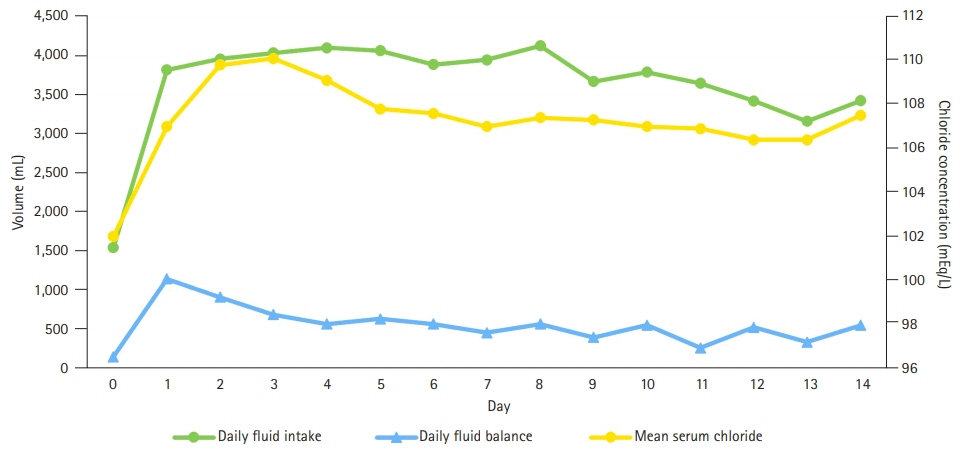
Fig. 2. Fluid intake, fluid balance, and serum chloride concentration by hospital day.

Fig. 3. Total fluid volume (A) and chloride dose (B) received, by category. IV, intravenous; IVPB, intravenous piggyback; MIVF, maintenance intravenous fluid.
Reference
-
1. Sadan O, Singbartl K, Kandiah PA, Martin KS, Samuels OB. Hyperchloremia is associated with acute kidney injury in patients with subarachnoid hemorrhage. Crit Care Med. 2017; 45:1382–8.
Article2. Patel VN, Samuels O. The critical care management of aneurysmal subarachnoid hemorrhage. In : Murai Y, editor. Aneurysm. Rijeka: IntechOpen;2012.3. Wartenberg KE, Schmidt JM, Claassen J, Temes RE, Frontera JA, Ostapkovich N, et al. Impact of medical complications on outcome after subarachnoid hemorrhage. Crit Care Med. 2006; 34:617–23.
Article4. van der Jagt M. Fluid management of the neurological patient: a concise review. Crit Care. 2016; 20:126.
Article5. Connolly ES Jr, Rabinstein AA, Carhuapoma JR, Derdeyn CP, Dion J, Higashida RT, et al. Guidelines for the management of aneurysmal subarachnoid hemorrhage: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2012; 43:1711–37.
Article6. Raabe A, Romner B. Hypervolemia in cerebral vasospasm. J Neurosurg. 2006; 104:994–5.
Article7. Neyra JA, Canepa-Escaro F, Li X, Manllo J, Adams-Huet B, Yee J, et al. Association of hyperchloremia with hospital mortality in critically ill septic patients. Crit Care Med. 2015; 43:1938–44.
Article8. Payen D, Haloui H. Acid-base status is an important factor for inflammation, but don’t forget CO2! Crit Care. 2014; 18:664.
Article9. Magee CA, Bastin MLT, Laine ME, Bissell BD, Howington GT, Moran PR, et al. Insidious harm of medication diluents as a contributor to cumulative volume and hyperchloremia: a prospective, open-label, sequential period pilot study. Crit Care Med. 2018; 46:1217–23.10. Rass V, Gaasch M, Kofler M, Schiefecker AJ, Ianosi BA, Steinkohl F, et al. Fluid intake but not fluid balance is associated with poor outcome in nontraumatic subarachnoid hemorrhage patients. Crit Care Med. 2019; 47:e555–62.
Article11. Sadan O, Singbartl K, Kraft J, Plancher JM, Greven AC, Kandiah P, et al. Low-chloride- versus high-chloride-containing hypertonic solution for the treatment of subarachnoid hemorrhage-related complications: the ACETatE (a low ChloriE hyperTonic solution for brain Edema) randomized trial. J Intensive Care. 2020; 8:32.12. Khwaja A. KDIGO clinical practice guidelines for acute kidney injury. Nephron Clin Pract. 2012; 120:c179–84.13. Büttner S, Stadler A, Mayer C, Patyna S, Betz C, Senft C, et al. Incidence, risk factors, and outcome of acute kidney injury in neurocritical care. J Intensive Care Med. 2020; 35:338–46.
Article14. Suarez JI, Qureshi AI, Parekh PD, Razumovsky A, Tamargo RJ, Bhardwaj A, et al. Administration of hypertonic (3%) sodium chloride/acetate in hyponatremic patients with symptomatic vasospasm following subarachnoid hemorrhage. J Neurosurg Anesthesiol. 1999; 11:178–84.15. Cook AM, Morgan Jones G, Hawryluk GW, Mailloux P, McLaughlin D, Papangelou A, et al. Guidelines for the acute treatment of cerebral edema in neurocritical care patients. Neurocrit Care. 2020; 32:647–66.
Article16. Macedo E, Bouchard J, Soroko SH, Chertow GM, Himmelfarb J, Ikizler TA, et al. Fluid accumulation, recognition and staging of acute kidney injury in critically-ill patients. Crit Care. 2010; 14:R82.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Frequency of Aneurysmal Subarachnoid Hemorrhage in Perimesencephalic Subarachnoid Hemorrhage and Need of 4-vessel Angiography
- Factors Related to Clinical Vasospasm after Aneurysmal Subarachnoid Hemorrhage
- Computerized Tomography Findings Suggesting Non-aneurysmal Spontaneous Subarachnoid Hemorrhage
- Simultaneous Occurrence of Aneurysmal Subarachnoid Hemorrhage and Hypertensive Intracerebral Hemorrhage
- Hemodynamics of Poor-grade Subarachnoid Hemorrhage
