Obesity and heart failure with preserved ejection fraction: pathophysiology and clinical significance
- Affiliations
-
- 1Division of Endocrinology and Metabolism, Department of Internal Medicine, Korea University Ansan Hospital, Korea University College of Medicine, Ansan, Korea
- KMID: 2536923
- DOI: http://doi.org/10.36011/cpp.2022.4.e10
Abstract
- Obesity is a risk factor for heart failure and cardiovascular disease. Of particular note, over 80% of patients with heart failure with a preserved ejection fraction (HFpEF) are overweight or obese. In this study, we aimed to review the association between obesity and HFpEF. Obese patients with HFpEF exhibit a distinct phenotype. In addition to impaired left ventricular (LV) diastolic function and high filling pressures, obese patients with HFpEF possess other factors that cause elevated LV filling pressure, such as a greater dependence on plasma volume expansion, aggravated pericardial restraint, and increased ventricular interaction. Obesity can contribute to HFpEF through hemodynamic, neurohormonal, inflammatory, and mechanical mechanisms. An increased amount of body fat can induce plasma volume expansion, resulting in chamber remodeling, pericardial restraint, and ultimately elevations in LV filling pressure. Obesity can mediate the activation of sympathetic nervous system signaling and the renin-angiotensin-aldosterone system. These unique pathophysiological characteristics of individuals with both obesity and HFpEF suggest that obesity with HFpEF can be considered a specific phenotype. Future research is expected to clarify effective treatment modalities for obesity-related HFpEF.
Keyword
Figure
-

Fig. 1. Positive correlations between the left heart filling pressure and (A) body mass and (B) plasma volume in obese heart failure with preserved ejection fraction (HFpEF) but not in nonobese HFpEF. PCWP, pulmonary capillary wedge pressure. Adapted from Obokata et al. [8] with permission from Wolters Kluwer Health Inc.
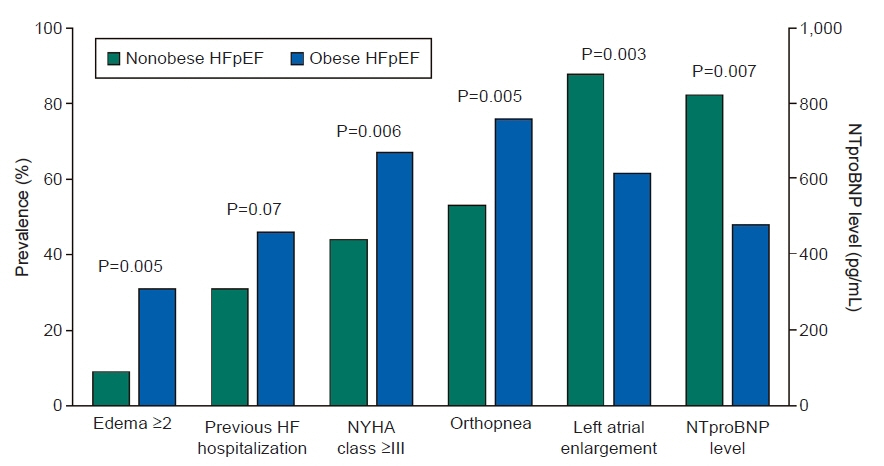
Fig. 2. Higher proportion of individuals suffering the symptoms and signs related to heart failure (HF) despite a lower prevalence of left atrial enlargement and lower levels of N-terminal pro B-type natriuretic peptide (NT-proBNP). HFpEF, heart failure with preserved ejection fraction; NYHA, New York Heart Association. Adapted from Reddy et al. [9] with permission from Elsevier.

Fig. 3. Adverse effects of obesity on the cardiovascular system in heart failure with preserved ejection fraction. LV, left ventricular; RV, right ventricular; RAAS, renin-angiotensin-aldosterone system; SNS, sympathetic nervous system; NO, nitric oxide; HFpEF, heart failure with preserved ejection fraction. Adapted from Harada et al. [1] with permission from Elsevier.
Reference
-
1. Harada T, Obokata M. Obesity-related heart failure with preserved ejection fraction: pathophysiology, diagnosis, and potential therapies. Heart Fail Clin. 2020; 16:357–68.2. Virani SS, Alonso A, Aparicio HJ, Benjamin EJ, Bittencourt MS, Callaway CW, et al. Heart disease and stroke statistics: 2021 update. A report from the American Heart Association. Circulation. 2021; 143:e254–743.3. Heidenreich PA, Albert NM, Allen LA, Bluemke DA, Butler J, Fonarow GC, et al. Forecasting the impact of heart failure in the United States: a policy statement from the American Heart Association. Circ Heart Fail. 2013; 6:606–19.4. Koliaki C, Liatis S, Kokkinos A. Obesity and cardiovascular disease: revisiting an old relationship. Metabolism. 2019; 92:98–107.
Article5. Ndumele CE, Matsushita K, Lazo M, Bello N, Blumenthal RS, Gerstenblith G, et al. Obesity and subtypes of incident cardiovascular disease. J Am Heart Assoc. 2016; 5:e003921.
Article6. Steinberg BA, Zhao X, Heidenreich PA, Peterson ED, Bhatt DL, Cannon CP, et al. Trends in patients hospitalized with heart failure and preserved left ventricular ejection fraction: prevalence, therapies, and outcomes. Circulation. 2012; 126:65–75.
Article7. Shah SJ, Kitzman DW, Borlaug BA, van Heerebeek L, Zile MR, Kass DA, et al. Phenotype-specific treatment of heart failure with preserved ejection fraction: a multiorgan roadmap. Circulation. 2016; 134:73–90.
Article8. Obokata M, Reddy Y, Pislaru SV, Melenovsky V, Borlaug BA. Evidence supporting the existence of a distinct obese phenotype of heart failure with preserved ejection fraction. Circulation. 2017; 136:6–19.
Article9. Reddy Y, Lewis GD, Shah SJ, Obokata M, Abou-Ezzedine OF, Fudim M, et al. Characterization of the obese phenotype of heart failure with preserved ejection fraction: a RELAX trial ancillary study. Mayo Clin Proc. 2019; 94:1199–209.
Article10. Turkbey EB, McClelland RL, Kronmal RA, Burke GL, Bild DE, Tracy RP, et al. The impact of obesity on the left ventricle: the Multi-Ethnic Study of Atherosclerosis (MESA). JACC Cardiovasc Imaging. 2010; 3:266–74.11. Wong CY, O'Moore-Sullivan T, Leano R, Byrne N, Beller E, Marwick TH. Alterations of left ventricular myocardial characteristics associated with obesity. Circulation. 2004; 110:3081–7.
Article12. Melenovsky V, Borlaug BA, Rosen B, Hay I, Ferruci L, Morell CH, et al. Cardiovascular features of heart failure with preserved ejection fraction versus nonfailing hypertensive left ventricular hypertrophy in the urban Baltimore community: the role of atrial remodeling/dysfunction. J Am Coll Cardiol. 2007; 49:198–207.
Article13. Packer M, Kitzman DW. Obesity-related heart failure with a preserved ejection fraction: the mechanistic rationale for combining inhibitors of aldosterone, neprilysin, and sodium-glucose cotransporter-2. JACC Heart Fail. 2018; 6:633–9.14. Wohlfahrt P, Redfield MM, Lopez-Jimenez F, Melenovsky V, Kane GC, Rodeheffer RJ, et al. Impact of general and central adiposity on ventricular-arterial aging in women and men. JACC Heart Fail. 2014; 2:489–99.15. Morricone L, Malavazos AE, Coman C, Donati C, Hassan T, Caviezel F. Echocardiographic abnormalities in normotensive obese patients: relationship with visceral fat. Obes Res. 2002; 10:489–98.
Article16. Selvaraj S, Martinez EE, Aguilar FG, Kim KY, Peng J, Sha J, et al. Association of central adiposity with adverse cardiac mechanics: findings from the Hypertension Genetic Epidemiology Network Study. Circ Cardiovasc Imaging. 2016; 9:10.1161/CIRCIMAGING.115.004396e004396.17. Licata G, Scaglione R, Barbagallo M, Parrinello G, Capuana G, Lipari R, et al. Effect of obesity on left ventricular function studied by radionuclide angiocardiography. Int J Obes. 1991; 15:295–302.18. Maurer MS, King DL, El-Khoury Rumbarger L, Packer M, Burkhoff D. Left heart failure with a normal ejection fraction: identification of different pathophysiologic mechanisms. J Card Fail. 2005; 11:177–87.
Article19. Hall JE, do Carmo JM, da Silva AA, Wang Z, Hall ME. Obesity-induced hypertension: interaction of neurohumoral and renal mechanisms. Circ Res. 2015; 116:991–1006.20. Lembo G, Vecchione C, Fratta L, Marino G, Trimarco V, d'Amati G, et al. Leptin induces direct vasodilation through distinct endothelial mechanisms. Diabetes. 2000; 49:293–7.
Article21. Gollasch M. Vasodilator signals from perivascular adipose tissue. Br J Pharmacol. 2012; 165:633–42.
Article22. Xie D, Bollag WB. Obesity, hypertension and aldosterone: is leptin the link? J Endocrinol. 2016; 230:F7–11.
Article23. Fudim M, Hernandez AF, Felker GM. Role of volume redistribution in the congestion of heart failure. J Am Heart Assoc. 2017; 6:e006817.
Article24. Chandra A, Neeland IJ, Berry JD, Ayers CR, Rohatgi A, Das SR, et al. The relationship of body mass and fat distribution with incident hypertension: observations from the Dallas Heart Study. J Am Coll Cardiol. 2014; 64:997–1002.
Article25. Standeven KF, Hess K, Carter AM, Rice GI, Cordell PA, Balmforth AJ, et al. Neprilysin, obesity and the metabolic syndrome. Int J Obes (Lond). 2011; 35:1031–40.
Article26. Foster MC, Hwang SJ, Porter SA, Massaro JM, Hoffmann U, Fox CS. Fatty kidney, hypertension, and chronic kidney disease: the Framingham Heart Study. Hypertension. 2011; 58:784–90.
Article27. Upadhya B, Haykowsky MJ, Kitzman DW. Therapy for heart failure with preserved ejection fraction: current status, unique challenges, and future directions. Heart Fail Rev. 2018; 23:609–29.
Article28. Pieske B, Tschope C, de Boer RA, Fraser AG, Anker SD, Donal E, et al. How to diagnose heart failure with preserved ejection fraction: the HFA-PEFF diagnostic algorithm: a consensus recommendation from the Heart Failure Association (HFA) of the European Society of Cardiology (ESC). Eur Heart J. 2019; 40:3297–317.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Heart failure with preserved ejection fraction: insights from recent clinical researches
- Optimal Management of Heart Failure with Preserve Ejection Fraction
- Obesity-related heart failure with preserved ejection fraction: diagnostic and therapeutic challenges
- Heart Failure with Preserved Ejection Fraction: the Major Unmet Need in Cardiology
- Simple and Practical Way of Assessing Diastolic Function: Diastolic Heart Failure Revisited
