A combined anterior and posterior approach for elbow ankylosis
- Affiliations
-
- 1Department of Orthopedic Surgery, National Police Hospital, Seoul, Korea
- 2Department of Orthopedic Surgery, Seoul National University Hospital, Seoul National University College of Medicine, Seoul, Korea
- 3Department of Orthopedic Surgery, SSMG-SNU Boramae Medical Center, Seoul National University College of Medicine, Seoul, Korea
- KMID: 2531920
- DOI: http://doi.org/10.12790/ahm.22.0001
Abstract
- Purpose
An ankylosed elbow should be released with consideration of the nature of the stiffness and location of the pathologic structures, and care should be taken to avoid damage to the surrounding musculature and neurovascular structures. We report the clinical results of a combined anterior and posterior approach, which allowed safe access with good visibility, for severe elbow stiffness.
Methods
We retrospectively reviewed patients who underwent surgical release for elbow ankylosis from August 2014 to May 2020. All operations were performed by the same surgeon at a single institution. The final outcomes were assessed by measuring the range of motion, calculating the Mayo Elbow Performance Score (MEPS), and reading radiologic images.
Results
Eight patients with a mean age of 43 years (range, 21–65 years) were included in the study, and the mean follow-up period was 22 months. The average range of motion was 13° of flexion contracture (range, 0°–40°) and 123° of further flexion (range, 100°–140°) at the last follow-up. The average net improvement in the total arc compared to patients’ preoperative status was 68° (range, –10°–130°). The mean postoperative MEPS was 89 points (range, 70–100 points). The development of heterotopic ossification and recalcitrant rheumatoid arthritis caused relatively poor outcomes.
Conclusion
The combined anterior and posterior approach allows safe access with good visibility for elbow ankylosis, while minimizing the risk of neurovascular injury and preserving the medial and lateral muscles.
Figure
-
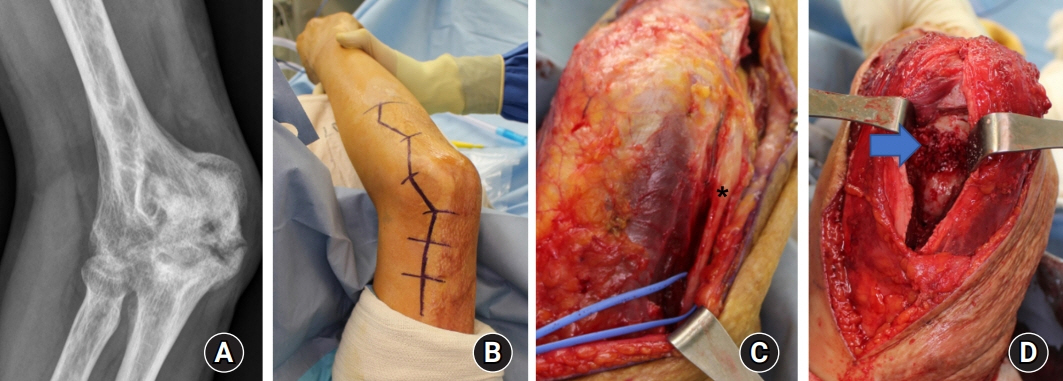
Fig. 1. A 51-year-old man with heterotopic ossification that occurred after a burn (patient 5). (A) Massive heterotopic ossification was observed in the olecranon fossa and posteromedial aspect of the elbow on preoperative X-rays. (B) The posterior incision was designed on the lateral side, avoiding an extensive burn scar at the medial aspect of the elbow. (C) The ulnar nerve (asterisk) was released, and the posteromedial aspect of the capsule was excised. (D) After removal of the large heterotopic ossification, the olecranon fossa (arrow) was exposed.

Fig. 2. A 25-year-old man with juvenile rheumatoid arthritis (patient 6) underwent extensive synovectomy through a combined anterior and posterior approach. (A) The thickened joint capsule was exposed via an anterior approach. (B) After synovectomy, the coronoid fossa (arrow) was exposed. (C, D) The triceps was detached from the posterior aspect of the humerus. Synovectomy was performed on the lateral side (B) and medial side (C), and the olecranon fossa (asterisk) was exposed (D).

Fig. 3. A 21-year-old woman with 60° flexion contracture (patient 8) underwent contracture release by an anterior approach. (A) The thickened lacertus fibrosus (arrow) was incised and anterior capsulectomy was performed. (B) During the process, the median nerve (asterisk) was identified and protected. (C) A full range of motion was achieved postoperatively.

Fig. 4. A 35-year-old woman with heterotopic ossification in her left elbow that occurred after surgical treatment for fractures of the distal humerus and the olecranon (patient 2). (A, B) Heterotopic ossification of the olecranon fossa and coronoid fossa was sufficiently removed. (C) Postoperatively, a range of motion close to normal was obtained.
Reference
-
References
1. Aldridge JM 3rd, Atkins TA, Gunneson EE, Urbaniak JR. Anterior release of the elbow for extension loss. J Bone Joint Surg Am. 2004; 86:1955–60.
Article2. Mih AD, Wolf FG. Surgical release of elbow-capsular contracture in pediatric patients. J Pediatr Orthop. 1994; 14:458–61.3. Morrey BF, Askew LJ, Chao EY. A biomechanical study of normal functional elbow motion. J Bone Joint Surg Am. 1981; 63:872–7.
Article4. Urbaniak JR, Hansen PE, Beissinger SF, Aitken MS. Correction of post-traumatic flexion contracture of the elbow by anterior capsulotomy. J Bone Joint Surg Am. 1985; 67:1160–4.
Article5. Willner P. Anterior capsulectomy for contractures of the elbow. J Int Coll Surg. 1948; 11:359–62.6. Cohen MS, Hastings H 2nd. Post-traumatic contracture of the elbow. Operative release using a lateral collateral ligament sparing approach. J Bone Joint Surg Br. 1998; 80:805–12.7. Husband JB, Hastings H 2nd. The lateral approach for operative release of post-traumatic contracture of the elbow. J Bone Joint Surg Am. 1990; 72:1353–8.
Article8. Mansat P, Morrey BF. The column procedure: a limited lateral approach for extrinsic contracture of the elbow. J Bone Joint Surg Am. 1998; 80:1603–15.9. Wada T, Ishii S, Usui M, Miyano S. The medial approach for operative release of post-traumatic contracture of the elbow. J Bone Joint Surg Br. 2000; 82:68–73.
Article10. Ruch DS, Shen J, Chloros GD, Krings E, Papadonikolakis A. Release of the medial collateral ligament to improve flexion in post-traumatic elbow stiffness. J Bone Joint Surg Br. 2008; 90:614–8.
Article11. Park MJ, Chang MJ, Lee YB, Kang HJ. Surgical release for posttraumatic loss of elbow flexion. J Bone Joint Surg Am. 2010; 92:2692–9.
Article12. Faber KJ, Patterson SD, King GJ. Post-traumatic elbow contracture release through a posterior midline longitudinal incision. J Bone Joint Surg. 1998; 80B:S6.13. Jones GS, Savoie FH 3rd. Arthroscopic capsular release of flexion contractures (arthrofibrosis) of the elbow. Arthroscopy. 1993; 9:277–83.
Article14. Kim SJ, Shin SJ. Arthroscopic treatment for limitation of motion of the elbow. Clin Orthop Relat Res. 2000; (375):140–8.
Article15. Noojin FK, Savoie FH 3rd, Field LD. Arthroscopic release of the stiff elbow. Tech Shoulder Elbow Surg. 2001; 2:17–25.
Article16. Darlis NA, Kaufmann RW, Sotereanos DG. Open surgical treatment of post-traumatic elbow contractures in adolescent patients. J Shoulder Elbow Surg. 2006; 15:709–15.
Article17. Koh KH, Lim TK, Lee HI, Park MJ. Surgical treatment of elbow stiffness caused by post-traumatic heterotopic ossification. J Shoulder Elbow Surg. 2013; 22:1128–34.
Article18. Morrey BF, An K, Chao E. Functional evaluation of the elbow. In : Morrey BF, editor. The elbow and its disorders. 3rd ed. Philadelphia: W.B. Saunders;2000. p. 74–157.19. Abrams GD, Bellino MJ, Cheung EV. Risk factors for development of heterotopic ossification of the elbow after fracture fixation. J Shoulder Elbow Surg. 2012; 21:1550–4.
Article20. Cai J, Wang W, Yan H, et al. Complications of open elbow arthrolysis in post-traumatic elbow stiffness: a systematic review. PLoS One. 2015; 10:e0138547.
Article21. Shin R, Ring D. The ulnar nerve in elbow trauma. J Bone Joint Surg Am. 2007; 89:1108–16.
Article22. Lindenhovius AL, Doornberg JN, Ring D, Jupiter JB. Health status after open elbow contracture release. J Bone Joint Surg Am. 2010; 92:2187–95.
Article23. Haglin JM, Kugelman DN, Christiano A, Konda SR, Paksima N, Egol KA. Open surgical elbow contracture release after trauma: results and recommendations. J Shoulder Elbow Surg. 2018; 27:418–26.
Article24. Haapaniemi T, Berggren M, Adolfsson L. Complete transection of the median and radial nerves during arthroscopic release of post-traumatic elbow contracture. Arthroscopy. 1999; 15:784–7.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Total Elbow Replacement
- Total Ankylosis by Heterotopic Ossification in an Adolescent Anterior Trans-olecranon Fracture Dislocation: A Case Report
- Total Elbow Arthroplasty for the Fracture of Elbow Arthrodesis Site: A Case Report
- Myositis Ossificans Traumatica Causing Ankylosis of the Elbow
- One Stage Three Column Fixation by Posterior Approach in Thoracolumbar Junction Lesion
