Hepatocyte Dysfunction in Patients with Nodular Goiter after Thyroidectomy Previously Received Hormone Suppressive Treatment
- Affiliations
-
- 1General Surgeon and Leading Scientific Researcher, Scientific Center of Surgery, Baku, Azerbaijan
- 2Endocrine Surgeon, Scientific Center of Surgery, Baku, Azerbaijan
- KMID: 2530124
- DOI: http://doi.org/10.11106/ijt.2022.15.1.36
Abstract
- Background and Objectives
Hepatic functions in patients with nodular goiter, who received long-term hormonal suppressive treatment was not well enlightened in publications. We studied liver specific enzymes activities in patients with nodular goiter after thyroidectomy. The aim of this study was comparative analysis of treatment outcomes of patients who were previously treated with L-thyroxine and were operated skipping hormonal treatment.
Materials and Methods
88 patients (basic group) with nodular goiter underwent surgical operation without any drug treatment. 86 patients in control group received hormonal suppressive treatment with L-thyroxine for 6-12 months and then underwent thyroidectomy. Liver ultrasound (US) scanning and laboratory tests were comparatively studied 3, 6, 12 months after thyroidectomy.
Results
Patients that received long-term hormonal suppressive treatment and then admitted for surgery, suffered from discomfort in upper right abdominal quadrant. The ALT, AST, Alkaline Phosphates and GGT activity of those patients was increased, and steatohepatitis was identified in US investigations. Also, total bilirubin, especially the unconjugated fraction concentration was higher in control group. The hepatocytes functional activity in basic group was slightly affected.
Conclusion
Long-term hormone suppressive therapy resulted in dysfunction of hepatocytes. It’s highly recommended to the patients with hormonal therapy resistant nodules to undergo surgical treatment.
Figure
-
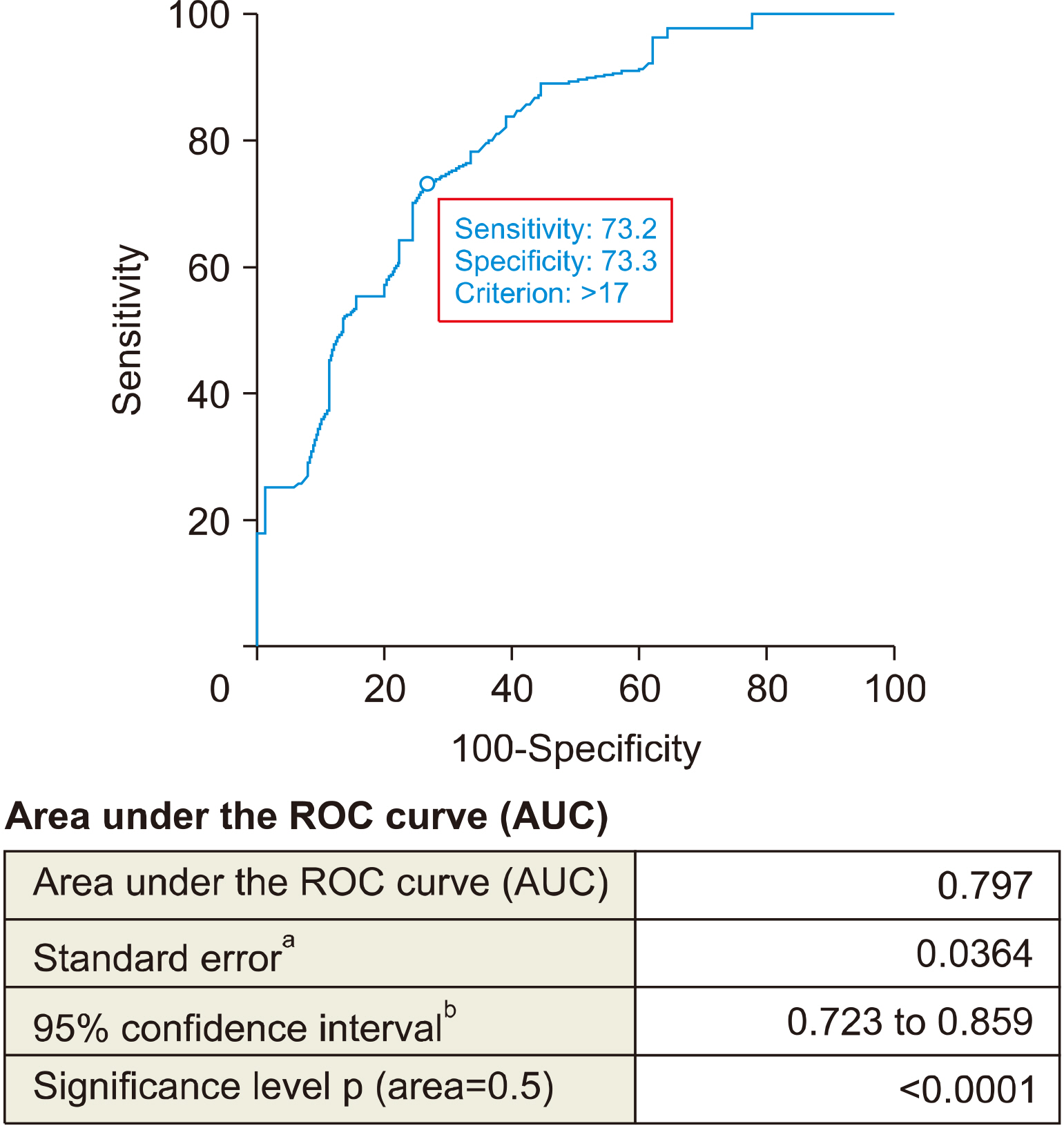
Fig. 1 ROC curve for measuring nodule size cut off value for defining resistant nodules to hormonal suppressive therapy.

Fig. 2 ROC curve for measuring thyroid gland volume cut off value for defining resistant nodules to hormonal suppressive therapy.
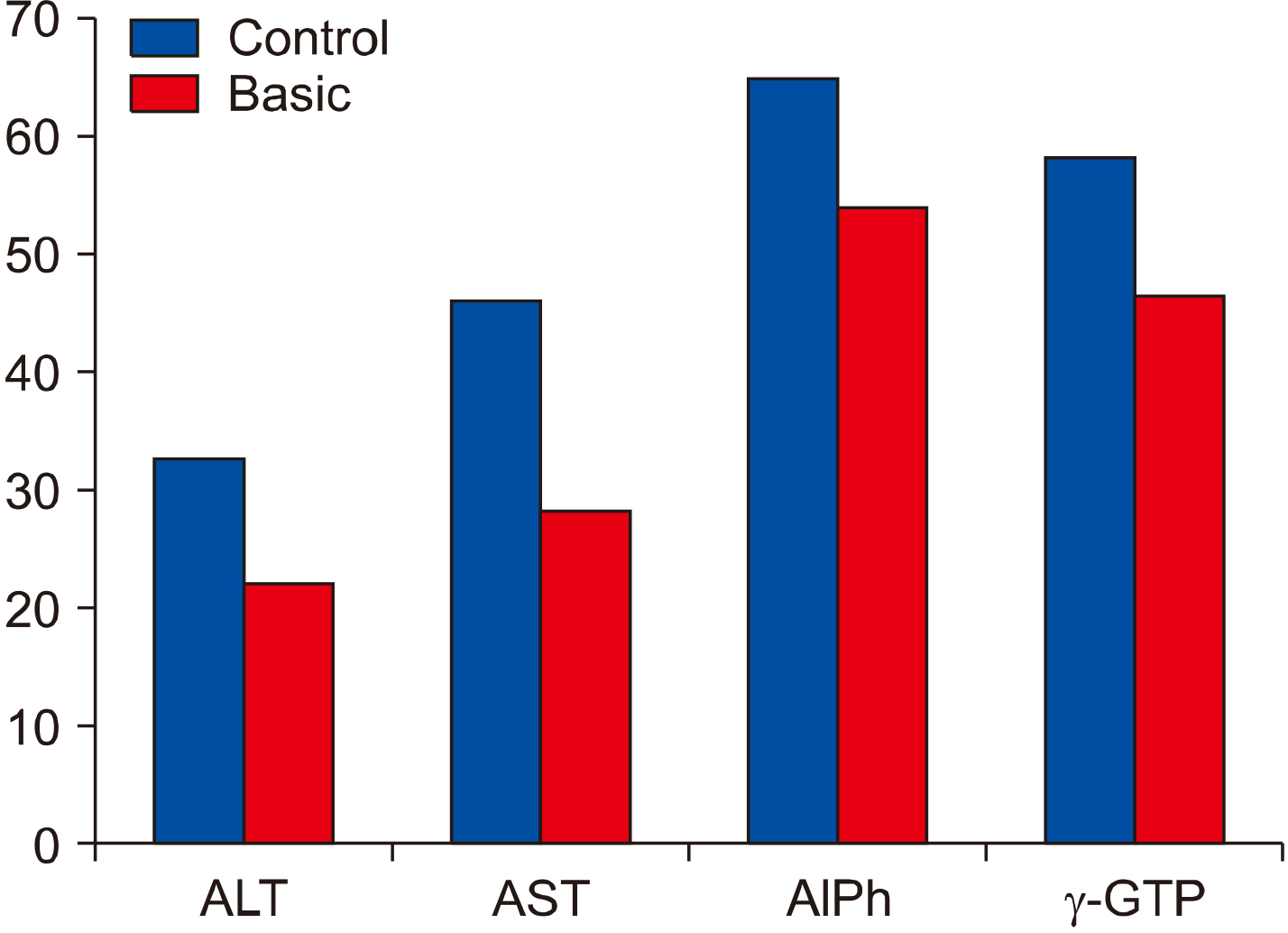
Fig. 3 Liver specific enzymes activity 3 months after surgery. AlPh: alkaline phosphatase, ALT: alanine amino-transferase, AST: aspartate aminotransferase, γ-GTP: γ- glutamyl transpeptidase
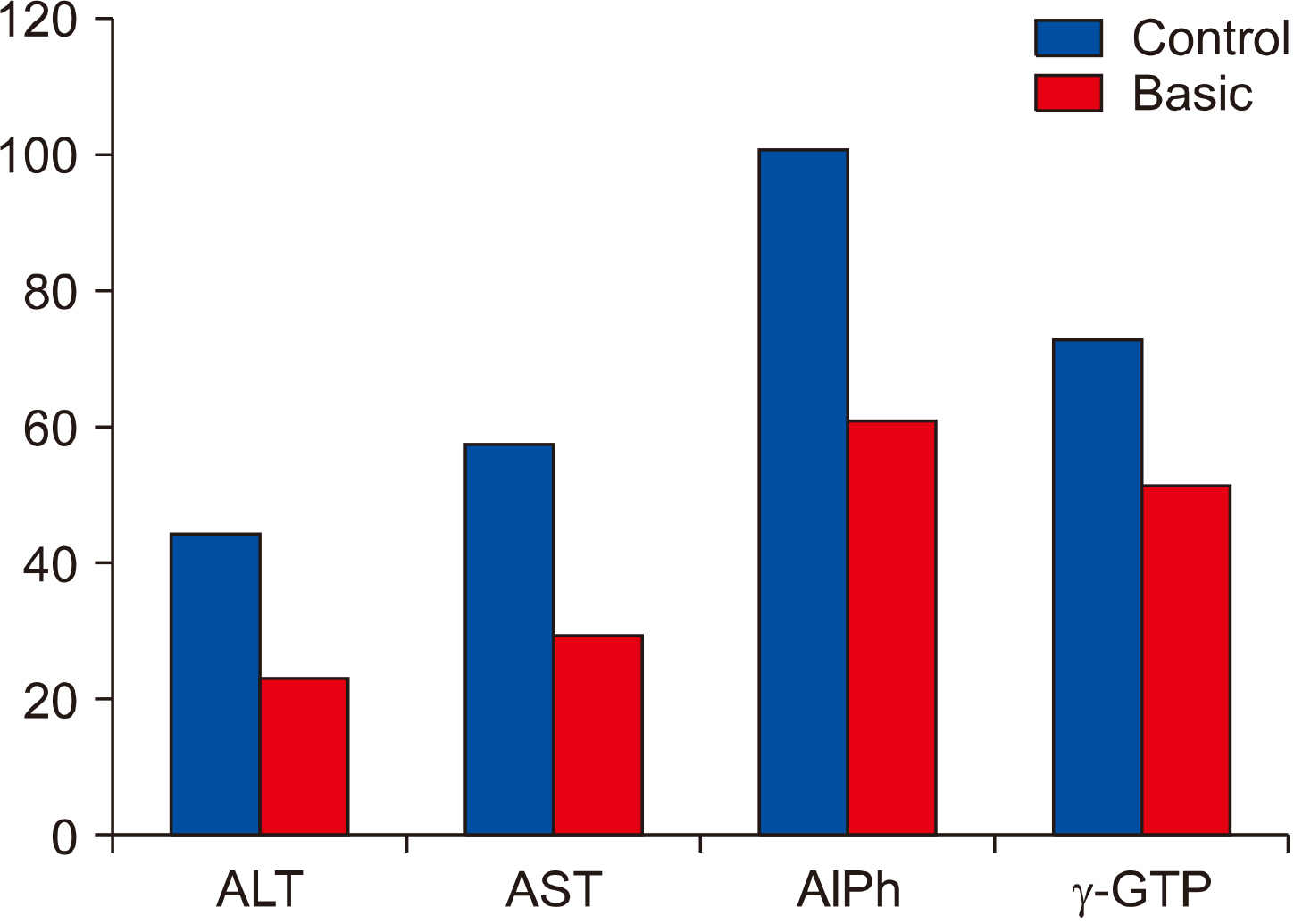
Fig. 4 Liver specific enzymes activity 6 months after surgery. AlPh: alkaline phosphatase, ALT: alanine amino-transferase, AST: aspartate aminotransferase, γ-GTP: γ- glutamyl transpeptidase
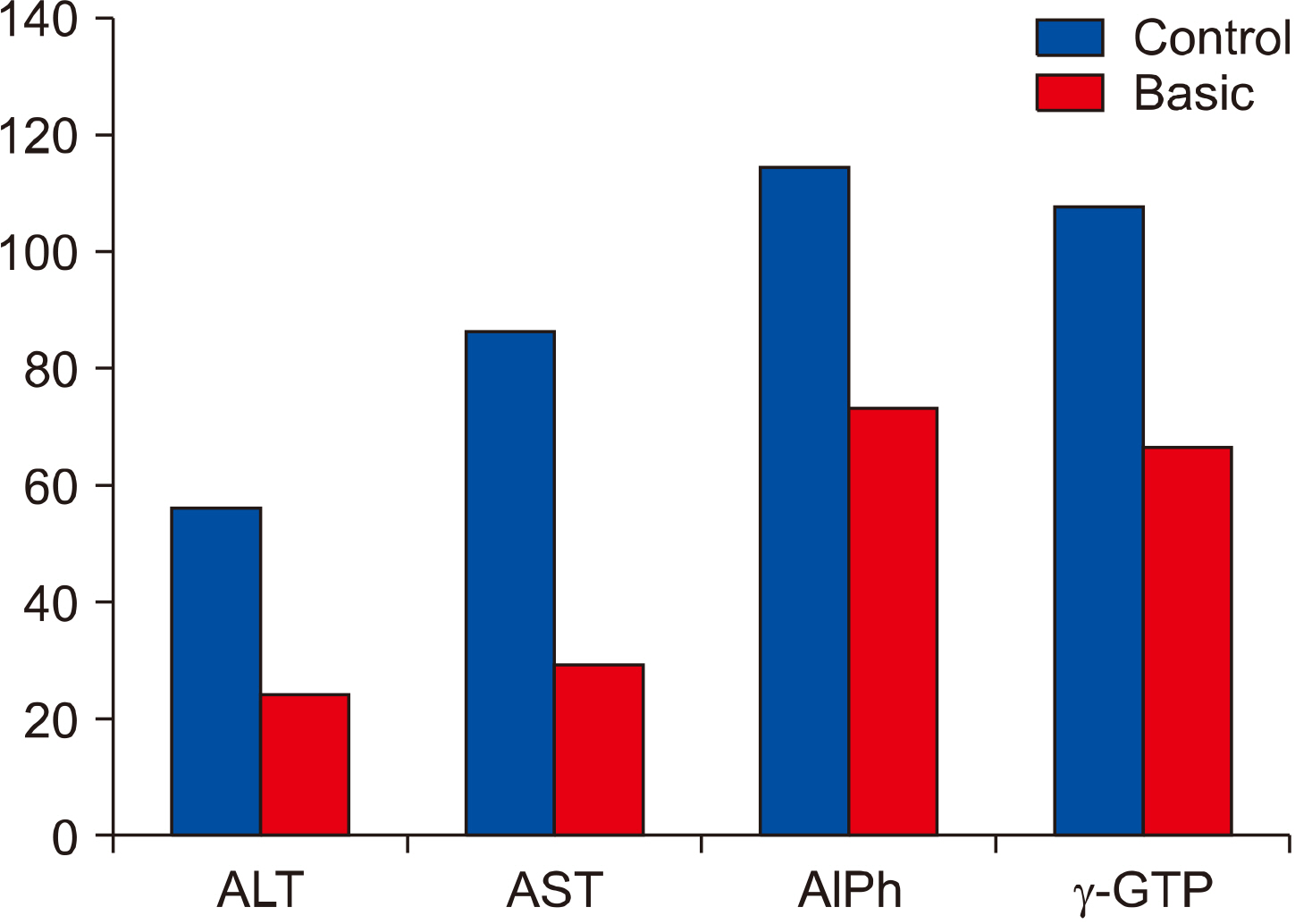
Fig. 5 Liver specific enzymes activity 12 months after surgery. AlPh: alkaline phosphatase, ALT: alanine amino-transferase, AST: aspartate aminotransferase, γ-GTP: γ- glutamyl transpeptidase
Reference
-
References
1. Walsh JP. 2016; Managing thyroid disease in general practice. Med J Aust. 205(4):179–84. DOI: 10.5694/mja16.00545. PMID: 27510349.
Article2. Knobel M. 2016; Etiopathology, clinical features, and treatment of diffuse and multinodular nontoxic goiters. J Endocrinol Invest. 39(4):357–73. DOI: 10.1007/s40618-015-0391-7. PMID: 26392367.
Article3. Chianelli M, Bizzarri G, Todino V, Misischi I, Bianchini A, Graziano F, et al. 2014; Laser ablation and 131-iodine: a 24-month pilot study of combined treatment for large toxic nodular goiter. J Clin Endocrinol Metab. 99(7):E1283–6. DOI: 10.1210/jc.2013-2967. PMID: 24684455.
Article4. Puzziello A, Carrano M, Angrisani E, Marotta V, Faggiano A, Zeppa P, et al. 2014; Evolution of benign thyroid nodules under levothyroxine non-suppressive therapy. J Endocrinol Invest. 37(12):1181–6. DOI: 10.1007/s40618-014-0128-z. PMID: 25008459.
Article5. Chen CY, Chen ST, Huang BY, Hwang JS, Lin JD, Liu FH. 2018; The effect of suppressive thyroxine therapy in nodular goiter in postmenopausal women and 2 year's bone mineral density change. Endocr J. 65(11):1101–9. DOI: 10.1507/endocrj.EJ18-0125. PMID: 30158361.
Article6. Miccoli P, Frustaci G, Fosso A, Miccoli M, Materazzi G. 2015; Surgery for recurrent goiter: complication rate and role of the thyroid-stimulating hormone-suppressive therapy after the first operation. Langenbecks Arch Surg. 400(2):253–8. DOI: 10.1007/s00423-014-1258-7. PMID: 25432523.
Article7. Appetecchia M. 2005; Effects on bone mineral density by treatment of benign nodular goiter with mildly suppressive doses of L-thyroxine in a cohort women study. Horm Res. 64(6):293–8. DOI: 10.1159/000089489. PMID: 16269872.8. Liu C, Lv H, Li Q, Fu S, Tan J, Wang C, et al. 2020; Effect of thyrotropin suppressive therapy on heart rate variability and QT dispersion in patients with differentiated thyroid cancer. Medicine (Baltimore). 99(28):e21190. DOI: 10.1097/MD.0000000000021190. PMID: 32664162. PMCID: PMC7360250.
Article9. Díaz-Fontenla F, Castillo-Pradillo M, Díaz-Gómez A, Ibanez-Samaniego L, Gancedo P, Guzman-de-Villoria JA, et al. 2017; Refractory hepatic encephalopathy in a patient with hypothyroidism: Another element in ammonia metabolism. World J Gastroenterol. 23(28):5246–52. DOI: 10.3748/wjg.v23.i28.5246. PMID: 28811719. PMCID: PMC5537191.
Article10. Hlaihel AF, Al-Khairalla MZH. 2019; Levothyroxine-induced liver injury followed by complete recovery upon cessation of the drug: a case report. J Med Case Rep. 13(1):311. DOI: 10.1186/s13256-019-2244-z. PMID: 31623668. PMCID: PMC6798352.
Article11. Yu H, Zhang W, Shen C, Zhang H, Zhang H, Zhang Y, et al. 2019; Liver dysfunction induced by Levothyroxine Sodium Tablets (Euthyrox(R)) in a hypothyroid patient with Hashimoto's thyroiditis: case report and literature review. Endocr J. 66(9):769–75. DOI: 10.1507/endocrj.EJ19-0078. PMID: 31217393.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Pendred's Syndrome
- Giant Multinodular Goiter, Mimicking a Direct Invasion from the Malignant Thyroid Neoplasm: A Case Report
- A Case Report of Severe Tracheal Compression Secondary to a Large Benign Substernal Goiter
- Changes of Thyroid Function in Patients Undergoing Partial Thyroidectomy for Benign Thyroid Tumors
- A Case of Unilateral Thyroid Agenesis with Contralateral Huge Goiter
