Feasibility and safety of endoscopic submucosal dissection for lesions in proximity to a colonic diverticulum
- Ikezawa N
 1
1 - Toyonaga T2,3
- Tanaka S1
- Yoshizaki T1
- Takao T1
- Abe H1
- Sakaguchi H1
- Tsuda K1
- Urakami S1
- Nakai T1
- Harada T4
- Miura K5
- Yamasaki T5
- Kostalas S6
- Morita Y1
- Kodama Y1
- Affiliations
-
- 1Division of Gastroenterology, Department of Internal Medicine, Graduate School of Medicine, Kobe University, Kobe, Japan
- 2Department of Endoscopy, Kobe University Hospital, Kobe, Japan
- 3Department of Gastroenterology, Kishiwada Tokushukai Hospital, Kishiwada, Japan
- 4Department of Gastroenterology, Teine Keijinkai Hospital, Sapporo, Japan
- 5Department of Gastroenterology, Yoka Municipal Hospital, Yabu, Japan
- 6Department of Gastroenterology, Port Macquarie Base Hospital, Port Macquarie, Australia
- KMID: 2529964
- DOI: http://doi.org/10.5946/ce.2021.245
Abstract
- Background/Aims
Endoscopic submucosal dissection (ESD) for diverticulum-associated colorectal lesions is generally contraindicated because of the high risk of perforation. Several studies on patients with such lesions treated with ESD have been reported recently. However, the feasibility and safety of ESD for lesions in proximity to a colonic diverticulum (D-ESD) have not been fully clarified. The aim of this study was to evaluate the feasibility and safety of D-ESD.
Methods
D-ESD was defined as ESD for lesions within approximately 3 mm of a diverticulum. Twenty-six consecutive patients who underwent D-ESD were included. Two strategic approaches were used depending on whether submucosal dissection of the diverticulum-related part was required (strategy B) or not (strategy A). Treatment outcomes and adverse events associated with each strategy were analyzed.
Results
The en bloc resection rate was 96.2%. The rates of R0 and curative resection in strategies A and B were 80.8%, 73.1%, 84.6%, and 70.6%, respectively. Two cases of intraoperative perforation and one case of delayed perforation occurred. The delayed perforation case required emergency surgery, but the other cases were managed conservatively.
Conclusions
D-ESD may be a feasible treatment option. However, it should be performed in a high-volume center by expert hands because it requires highly skilled endoscopic techniques.
Keyword
Figure
-
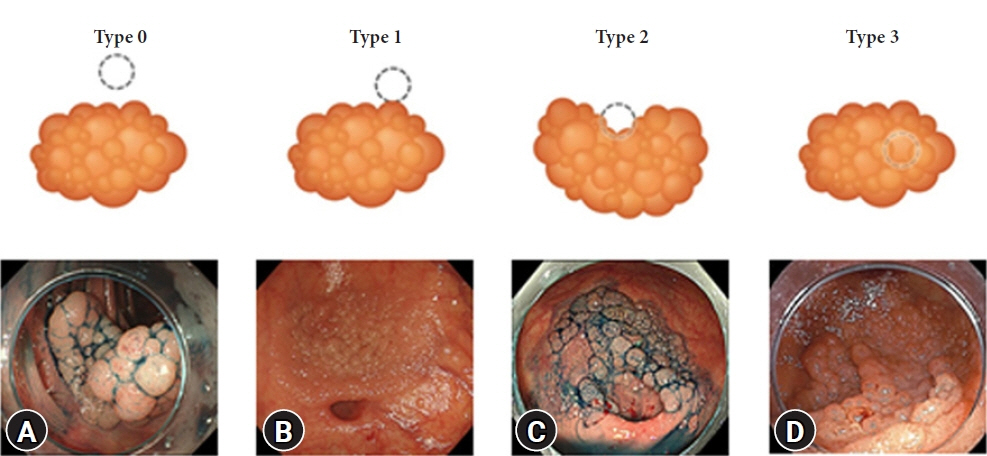
Fig. 1. Classification according to the association between a lesion and a diverticulum. (A) Type 0: a lesion within 3 mm of the diverticulum border. However, a normal mucosa intervens between the diverticulum and the lesion. (B) Type 1: a lesion reaches the border of the diverticulum but does not involve the orifice of the diverticulum. (C) Type 2: a lesion reaches and partially involves the orifice of the diverticulum. (D) Type 3: a lesion completely covers the orifice of the diverticulum. In some cases, the presence of a diverticulum cannot be recognized preoperatively.
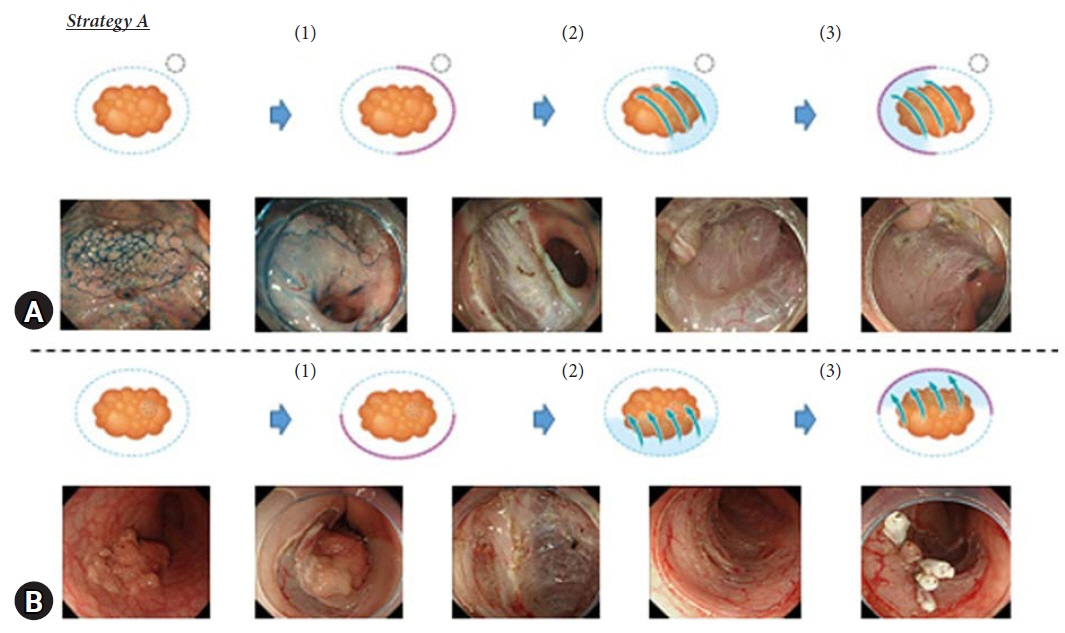
Fig. 2. Strategic approach for endoscopic submucosal dissection of lesions in proximity to a colonic diverticulum. Strategy A for type 0 and some type 1 and type 3 lesions. (1) A semi-circumferential mucosal incision was made between the lesion and the diverticulum or from the anal side of the lesion. (2) Submucosal dissection was performed on the anal side towards the oral side. (3) A circumferential incision and submucosal dissection were performed in the remaining parts. Dot circle, diverticulum; red line, mucosal incision; blue arrow, submucosal dissection.
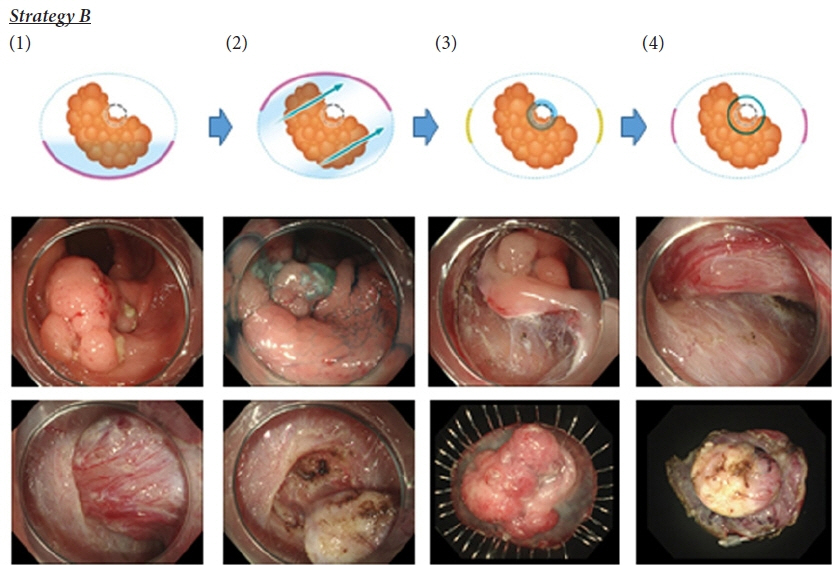
Fig. 3. Strategic approach for endoscopic submucosal dissection of lesions in proximity to a colonic diverticulum. Strategy B for type 2 lesions and some type 1 and type 3 lesions. (1) A semi-circumferential mucosal incision was made from the anal side of the lesion. (2) Submucosal dissection was performed, and double pockets were made on both sides of the diverticulum towards the oral side. (3) Submucosal dissection around the diverticulum was performed maximally to expose the diverticulum under the lesion. Mucosae on both lateral sides were left at this time (yellow line). (4) Dissection of the diverticulum was performed carefully using the tapping technique, and the remaining mucosal incision was then completed. Dot circle, diverticulum; red line, mucosal incision; blue arrow, submucosal dissection.
Reference
-
1. Nagata N, Niikura R, Aoki T, et al. Increase in colonic diverticulosis and diverticular hemorrhage in an aging society: lessons from a 9-year colonoscopic study of 28,192 patients in Japan. Int J Colorectal Dis. 2014; 29:379–385.2. Fu KI, Hamahata Y, Tsujinaka Y. Early colon cancer within a diverticulum treated by magnifying chromoendoscopy and laparoscopy. World J Gastroenterol. 2010; 16:1545–1547.3. Saito Y, Uraoka T, Yamaguchi Y, et al. A prospective, multicenter study of 1111 colorectal endoscopic submucosal dissections (with video). Gastrointest Endosc. 2010; 72:1217–1225.4. Repici A, Hassan C, De Paula Pessoa D, et al. Efficacy and safety of endoscopic submucosal dissection for colorectal neoplasia: a systematic review. Endoscopy. 2012; 44:137–150.5. Tanaka S, Terasaki M, Kanao H, et al. Current status and future perspectives of endoscopic submucosal dissection for colorectal tumors. Dig Endosc. 2012; 24(Suppl 1):73–79.6. Jacob H, Toyonaga T, Ohara Y, et al. Endoscopic submucosal dissection of cecal lesions in proximity to the appendiceal orifice. Endoscopy. 2016; 48:829–836.7. Yoshizaki T, Toyonaga T, Tanaka S, et al. Feasibility and safety of endoscopic submucosal dissection for lesions involving the ileocecal valve. Endoscopy. 2016; 48:639–645.8. Kobara H, Mori H, Rafiq K, et al. A peripheral approach allowing successful endoscopic submucosal dissection for early colorectal carcinoma near the diverticula. Rev Esp Enferm Dig. 2015; 107:378–379.9. Ritsuno H, Sakamoto N, Osada T, et al. Large superficial tumor of the colon involving a diverticulum removed by endoscopic submucosal dissection. Gastrointest Endosc. 2015; 82:751.10. Sakamoto T, Abe S, Nakajima T, et al. Complete removal of a colonic neoplasm extending into a diverticulum with hybrid endoscopic submucosal dissection-mucosal resection and endoscopic band ligation. Endoscopy. 2015; 47(Suppl 1 UCTN):E295–E296.11. Kato M, Uraoka T, Wada M, et al. Laterally spreading tumor involving a colon diverticulum successfully resected by endoscopic submucosal dissection. Gastrointest Endosc. 2016; 84:191–192.12. Iwatsubo T, Uedo N, Yamasaki Y, et al. Traction-assisted colorectal endoscopic submucosal dissection by use of clip and line for a neoplasm involving colonic diverticulum. VideoGIE. 2017; 2:337–338.13. Takasago T, Kuwai T, Yamaguchi T, et al. Endoscopic submucosal dissection with a scissors-type knife for post-EMR recurrence tumor involving the colon diverticulum. VideoGIE. 2017; 2:211–212.14. Yoshida N, Naito Y, Kishimoto M. Endoscopic submucosal dissection of T1 cancer with colonic diverticulum by pocket-creation method. Dig Endosc. 2017; 29:726–727.15. Jimenez-Garcia VA, Yamada M, Ikematsu H, et al. Endoscopic submucosal dissection in management of colorectal tumors near or involving a diverticulum: a retrospective case series. Endosc Int Open. 2019; 7:E664–E671.16. Tanaka S, Kashida H, Saito Y, et al. JGES guidelines for colorectal endoscopic submucosal dissection/endoscopic mucosal resection. Dig Endosc. 2015; 27:417–434.17. Yamamoto K, Hayashi S, Saiki H, et al. Endoscopic submucosal dissection for large superficial colorectal tumors using the "clip-flap method". Endoscopy. 2015; 47:262–265.18. Sakamoto H, Hayashi Y, Miura Y, et al. Pocket-creation method facilitates endoscopic submucosal dissection of colorectal laterally spreading tumors, non-granular type. Endosc Int Open. 2017; 5:E123–E129.19. Ishida T, Jacob H, Toyonaga T. The goals and pitfalls of gastric submucosal dissection: a special focus on dissection of lesions with severe fibrosis. Korean J Helicobacter Up Gastrointest Res. 2014; 14:163–173.20. Toyonaga T, Man IM, Fujita T, et al. The performance of a novel ball-tipped Flush knife for endoscopic submucosal dissection: a case-control study. Aliment Pharmacol Ther. 2010; 32:908–915.21. Takezawa T, Hayashi Y, Shinozaki S, et al. The pocket-creation method facilitates colonic endoscopic submucosal dissection (with video). Gastrointest Endosc. 2019; 89:1045–1053.22. Ritsuno H, Sakamoto N, Osada T, et al. Prospective clinical trial of traction device-assisted endoscopic submucosal dissection of large superficial colorectal tumors using the S-O clip. Surg Endosc. 2014; 28:3143–3149.23. Yamasaki Y, Takeuchi Y, Hanaoka N, et al. A novel traction method using an endoclip attached to a nylon string during colonic endoscopic submucosal dissection. Endoscopy. 2015; 47(Suppl 1 UCTN):E238–E239.24. Okamoto Y, Oka S, Tanaka S, et al. Clinical usefulness of the S-O clip during colorectal endoscopic submucosal dissection in difficult-to-access submucosal layer. Endosc Int Open. 2020; 8:E437–E444.25. Muramoto T, Ohata K, Sakai E, et al. Endoscopic submucosal dissection for colorectal neoplasms in proximity or extending to a diverticulum. Surg Endosc. 2021; 35:3479–3487.26. Valli PV, Kaufmann M, Vrugt B, et al. Endoscopic resection of a diverticulum-arisen colonic adenoma using a full-thickness resection device. Gastroenterology. 2014; 147:969–971.27. Shakhatreh MH, Hair C, Shaib YH, et al. Removal of a colonic polyp in a diverticulum: a novel use of the over-the-scope clip device. Gastrointest Endosc. 2015; 81:756.28. Isohata N, Nagata K, Utano K, et al. Recent trends in the prevalence and distribution of colonic diverticular in Japan evaluated using computed tomography colonography. World J Gastroenterol. 2021; 27:4441–4452.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Underwater Endoscopic Mucosal Resection without Submucosal Injection Facilitates En bloc Resection of Colon Adenomas Extending into a Diverticulum
- Successful Endoscopic Resection of Residual Colonic Mucosa-Associated Lymphoid Tissue Lymphoma after Polypectomy
- Endoscopic Treatment of Subepithelial Tumors
- Endoscopic Submucosal Dissection of an Inverted Early Gastric Cancer-Forming False Gastric Diverticulum
- History and Development of Accessories for Endoscopic Submucosal Dissection
