Electrical Remodeling of Left Atrium Is a Better Predictor for Recurrence Than Structural Remodeling in Atrial Fibrillation Patients Undergoing Radiofrequency Catheter Ablation
- Affiliations
-
- 1Arrhythmia Center, Korea University Medicine Anam Hospital, Seoul, Korea
- KMID: 2529868
- DOI: http://doi.org/10.4070/kcj.2021.0323
Abstract
- Background and Objectives
Recurrence rates after radiofrequency catheter ablation (RFCA) in atrial fibrillation (AF) patients are not low especially in non-paroxysmal AF. The diameter of left atrium (LA) has been widely used to predict the recurrence after RFCA for decades. However, LA diameter represents structural remodeling of LA and does not reflect electrical remodeling. We aimed to determine the predictive value of electrical remodeling of LA which is represented by the amount of low voltage zone (LVZ).
Methods
We performed a retrospective cohort analysis of AF patients who underwent de novo RFCA in a single-center.
Results
A total of 3,120 AF patients with de novo RFCA were analyzed. Among these patients, 537 patients underwent an electroanatomic mapping with bipolar voltage measurement of LA. The diameter of LA and flow velocity of LA appendage (LAA) differed significantly according to quartile group of LVZ area and percentage: patients with high LVZ had large LA diameter and low LAA flow velocity (p<0.001). Freedom from late recurrence (LR) was significantly lower in patients with high LVZ area and percentage (p<0.001). The diameter and surface area of LA had area under curve (AUC) of 0.592 and 0.593, respectively (p=0.002 for both). The predictive value of LVZ area (AUC, 0.676) and percentage (AUC, 0.671) were both superior compared with LA diameter (p=0.011 and 0.027 for each comparison).
Conclusions
In conclusion, LVZ can predict freedom from LR after RFCA in AF patients. Predictive value was higher in parameters reflecting electrical rather than structural remodeling of LA.
Keyword
Figure
-

Figure 1 Flow of the study.LA = left atrium; LVZ = low voltage zone; RFCA = radiofrequency catheter ablation.

Figure 2 Association between LVZ and echocardiographic findings. (A) Difference in LA diameter according to LVZ area quartile. (B) Difference in LA diameter according to LVZ percentage quartile. (C) Difference in LAAFV according to LVZ area quartile. (D) Difference in LAAFV according to LVZ percentage quartile.LA = left atrium; LAAFV = left atrial flow velocity; LVZ = low voltage zone.
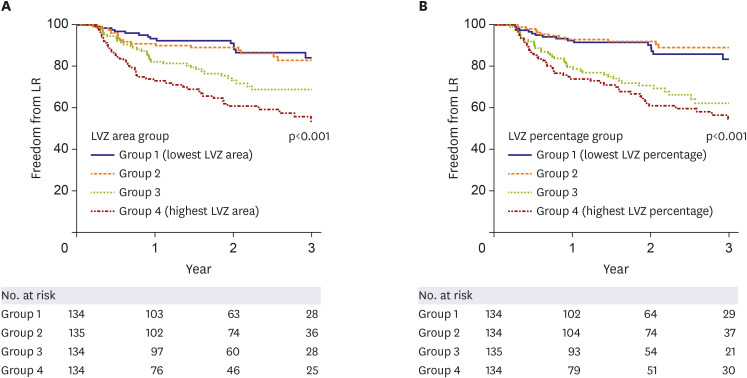
Figure 3 Impact of LVZ on LR. (A) Freedom from LR was significantly affected by LVZ area quartile. The p value for (i) group 1 vs. group 2=0.774; (ii) group 1 vs. group 3=0.001; (iii) group 1 vs. group 4<0.001; (iv) group 2 vs. group 3=0.004; (v) group 2 vs. group 4<0.001; (vi) group 3 vs. group 4=0.054. (B) Freedom from late recurrence LR was significantly affected by LVZ percentage quartile. The p value for (i) group 1 vs. group 2=0.567; (ii) group 1 vs. group 3<0.001; (iii) group 1 vs. group 4<0.001; (iv) group 2 vs. group 3<0.001; (v) group 2 vs. group 4<0.001; (vi) group 3 vs. group 4=0.318.LR = late recurrence; LVZ = low voltage zone.
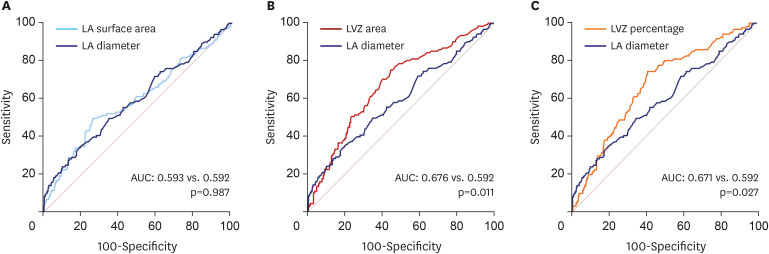
Figure 4 Electrical remodeling vs. structural remodeling. (A) LA diameter and LA surface area showed similar predictive value for late recurrence. (B) LVZ area had significantly higher predictive value compared with LA diameter. (C) LVZ percentage had significantly higher predictive value compared with LA diameter.AUC = area under curve; LA = left atrium; LVZ = low voltage zone.
Cited by 3 articles
-
What Is Better Predictor of Late Recurrence after Radiofrequency Catheter Ablation for Atrial Fibrillation?
Sung Il Im, Kyoung-Min Park
Korean Circ J. 2022;52(5):379-381. doi: 10.4070/kcj.2022.0008.The Impact of Right Atrial Size to Predict Success of Direct Current Cardioversion in Patients With Persistent Atrial Fibrillation
Christoph Döring, Utz Richter, Stefan Ulbrich, Carsten Wunderlich, Micaela Ebert, Sergio Richter, Axel Linke, Krunoslav Michael Sveric
Korean Circ J. 2023;53(5):331-343. doi: 10.4070/kcj.2022.0291.Can Current Subclinical Atrial Fibrillation Be Verified by P Wave of 12-Lead ECG at Present? The Answer Already Exists in the Atrial Substrate
Seung Yong Shin
Korean Circ J. 2023;53(9):632-634. doi: 10.4070/kcj.2023.0188.
Reference
-
1. Go AS, Hylek EM, Phillips KA, et al. Prevalence of diagnosed atrial fibrillation in adults: national implications for rhythm management and stroke prevention: the AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. JAMA. 2001; 285:2370–2375. PMID: 11343485.
Article2. Miyasaka Y, Barnes ME, Gersh BJ, et al. Secular trends in incidence of atrial fibrillation in Olmsted County, Minnesota, 1980 to 2000, and implications on the projections for future prevalence. Circulation. 2006; 114:119–125. PMID: 16818816.
Article3. Corley SD, Epstein AE, DiMarco JP, et al. Relationships between sinus rhythm, treatment, and survival in the Atrial Fibrillation Follow-Up Investigation of Rhythm Management (AFFIRM) Study. Circulation. 2004; 109:1509–1513. PMID: 15007003.
Article4. Wyse DG, Waldo AL, DiMarco JP, et al. A comparison of rate control and rhythm control in patients with atrial fibrillation. N Engl J Med. 2002; 347:1825–1833. PMID: 12466506.
Article5. Wilber DJ, Pappone C, Neuzil P, et al. Comparison of antiarrhythmic drug therapy and radiofrequency catheter ablation in patients with paroxysmal atrial fibrillation: a randomized controlled trial. JAMA. 2010; 303:333–340. PMID: 20103757.
Article6. Packer DL, Mark DB, Robb RA, et al. Effect of catheter ablation vs antiarrhythmic drug therapy on mortality, stroke, bleeding, and cardiac arrest among patients with atrial fibrillation: the cabana randomized clinical trial. JAMA. 2019; 321:1261–1274. PMID: 30874766.7. Pappone C, Augello G, Sala S, et al. A randomized trial of circumferential pulmonary vein ablation versus antiarrhythmic drug therapy in paroxysmal atrial fibrillation: the APAF Study. J Am Coll Cardiol. 2006; 48:2340–2347. PMID: 17161267.
Article8. Marrouche NF, Brachmann J, Andresen D, et al. Catheter ablation for atrial fibrillation with heart failure. N Engl J Med. 2018; 378:417–427. PMID: 29385358.
Article9. Verma A, Jiang CY, Betts TR, et al. Approaches to catheter ablation for persistent atrial fibrillation. N Engl J Med. 2015; 372:1812–1822. PMID: 25946280.
Article10. Kim YG, Choi JI, Boo KY, et al. Clinical and echocardiographic risk factors predict late recurrence after radiofrequency catheter ablation of atrial fibrillation. Sci Rep. 2019; 9:6890. PMID: 31053744.
Article11. Yamaguchi T, Tsuchiya T, Fukui A, et al. Impact of the extent of low-voltage zone on outcomes after voltage-based catheter ablation for persistent atrial fibrillation. J Cardiol. 2018; 72:427–433. PMID: 29807864.
Article12. Rolf S, Kircher S, Arya A, et al. Tailored atrial substrate modification based on low-voltage areas in catheter ablation of atrial fibrillation. Circ Arrhythm Electrophysiol. 2014; 7:825–833. PMID: 25151631.
Article13. Marrouche NF, Wilber D, Hindricks G, et al. Association of atrial tissue fibrosis identified by delayed enhancement MRI and atrial fibrillation catheter ablation: the DECAAF study. JAMA. 2014; 311:498–506. PMID: 24496537.
Article14. Kircher S, Arya A, Altmann D, et al. Individually tailored vs. standardized substrate modification during radiofrequency catheter ablation for atrial fibrillation: a randomized study. Europace. 2018; 20:1766–1775. PMID: 29177475.
Article15. Verma A, Wazni OM, Marrouche NF, et al. Pre-existent left atrial scarring in patients undergoing pulmonary vein antrum isolation: an independent predictor of procedural failure. J Am Coll Cardiol. 2005; 45:285–292. PMID: 15653029.
Article16. Kim YG, Shim J, Kim DH, et al. Characteristics of atrial fibrillation patients suffering atrioesophageal fistula after radiofrequency catheter ablation. J Cardiovasc Electrophysiol. 2018; 29:1343–1351. PMID: 29927012.
Article17. Kim YG, Han S, Choi JI, et al. Impact of persistent left superior vena cava on radiofrequency catheter ablation in patients with atrial fibrillation. Europace. 2019; 21:1824–1832. PMID: 31578551.
Article18. Kim YG, Han KD, Choi JI, et al. Non-genetic risk factors for atrial fibrillation are equally important in both young and old age: a nationwide population-based study. Eur J Prev Cardiol. 2021; 28:666–676. PMID: 34021574.
Article19. Hanley JA, McNeil BJ. A method of comparing the areas under receiver operating characteristic curves derived from the same cases. Radiology. 1983; 148:839–843. PMID: 6878708.
Article20. Kim YG, Shim J, Oh SK, Lee KN, Choi JI, Kim YH. Risk factors for ischemic stroke in atrial fibrillation patients undergoing radiofrequency catheter ablation. Sci Rep. 2019; 9:7051. PMID: 31065030.
Article21. Lee KN, Roh SY, Baek YS, et al. Long-term clinical comparison of procedural end points after pulmonary vein isolation in paroxysmal atrial fibrillation: Elimination of nonpulmonary vein triggers versus noninducibility. Circ Arrhythm Electrophysiol. 2018; 11:e005019. PMID: 29431632.
Article22. Haldar S, Khan HR, Boyalla V, et al. Catheter ablation vs. thoracoscopic surgical ablation in long-standing persistent atrial fibrillation: CASA-AF randomized controlled trial. Eur Heart J. 2020; 41:4471–4480. PMID: 32860414.
Article23. Corradi D, Callegari S, Maestri R, Benussi S, Alfieri O. Structural remodeling in atrial fibrillation. Nat Clin Pract Cardiovasc Med. 2008; 5:782–796. PMID: 18852714.
Article24. Corradi D. Atrial fibrillation from the pathologist’s perspective. Cardiovasc Pathol. 2014; 23:71–84. PMID: 24462196.
Article25. Allessie MA, de Groot NM, Houben RP, et al. Electropathological substrate of long-standing persistent atrial fibrillation in patients with structural heart disease: longitudinal dissociation. Circ Arrhythm Electrophysiol. 2010; 3:606–615. PMID: 20719881.
Article26. Myerburg RJ, Nilsson K, Befeler B, Castellanos A Jr, Gelband H. Transverse spread and longitudinal dissociation in the distal A-V conducting system. J Clin Invest. 1973; 52:885–895. PMID: 4693653.
Article27. Masuda M, Fujita M, Iida O, et al. Influence of underlying substrate on atrial tachyarrhythmias after pulmonary vein isolation. Heart Rhythm. 2016; 13:870–878. PMID: 26711800.
Article28. Matsuda Y, Masuda M, Asai M, et al. A new clinical risk score for predicting the prevalence of low-voltage areas in patients undergoing atrial fibrillation ablation. J Cardiovasc Electrophysiol. 2020; 31:3150–3158. PMID: 32966648.
Article29. Sanders P, Morton JB, Davidson NC, et al. Electrical remodeling of the atria in congestive heart failure: electrophysiological and electroanatomic mapping in humans. Circulation. 2003; 108:1461–1468. PMID: 12952837.
Article30. Yang B, Jiang C, Lin Y, et al. STABLE-SR (electrophysiological substrate ablation in the left atrium during sinus rhythm) for the treatment of nonparoxysmal atrial fibrillation: a prospective, multicenter randomized clinical trial. Circ Arrhythm Electrophysiol. 2017; 10:e005405. PMID: 29141843.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Successful Ablation of Right-Sided Accessory Pathway during Atrial Fibrillation
- The Impact of the CHAâ‚‚DSâ‚‚-VASc Score on Recurrence of Atrial Fibrillation after a Single Catheter Ablation and Atrial Remodeling in Patients with Non-Valvular Atrial Fibrillation
- Relationship between Epicardial Fat Accumulation and Left Atrial Reverse Remodeling after Catheter Ablation of Atrial Fibrillation
- A Case of Chronic Radiodermatitis following Radiofrequency Catheter Ablation for Atrial Fibrillation
- Catheter Ablation of Long-standing Persistent Atrial Fibrillation: a Reckless Challenge or a Way to Real Cure?
