Korean J Gastroenterol.
2022 Mar;79(3):126-129. 10.4166/kjg.2022.018.
Gastric Ectopic Pyloric Opening with Gastric Ulcer: A Rare Case
- Affiliations
-
- 1Department of Internal Medicine, Dong-A University College of Medicine, Busan, Korea
- KMID: 2527480
- DOI: http://doi.org/10.4166/kjg.2022.018
Abstract
- The stomach temporarily stores food and secretes gastric juices to break down and digest food. The normal process is the movement of food digested from the stomach to the duodenum, with the pylorus as a passageway. This paper reports the case of a patient with an ectopic gastric pylorus who presented with gastrointestinal bleeding. A 62-year-old man complained of melena with mild dizziness and nausea. An endoscopic examination revealed a gastric ulcer, approximately 1 cm in diameter, and exposed blood vessels on the posterior wall of the upper body. No normal pyloric structure was observed in the distal antrum, and an opening leading to the duodenum was noted in the posterior wall of the upper body adjacent to the ulcer. This case presents a congenital pyloric ectopic opening in the upper body of the stomach, not in the distal antrum, suggesting a rare gastric morphological variation.
Keyword
Figure
-
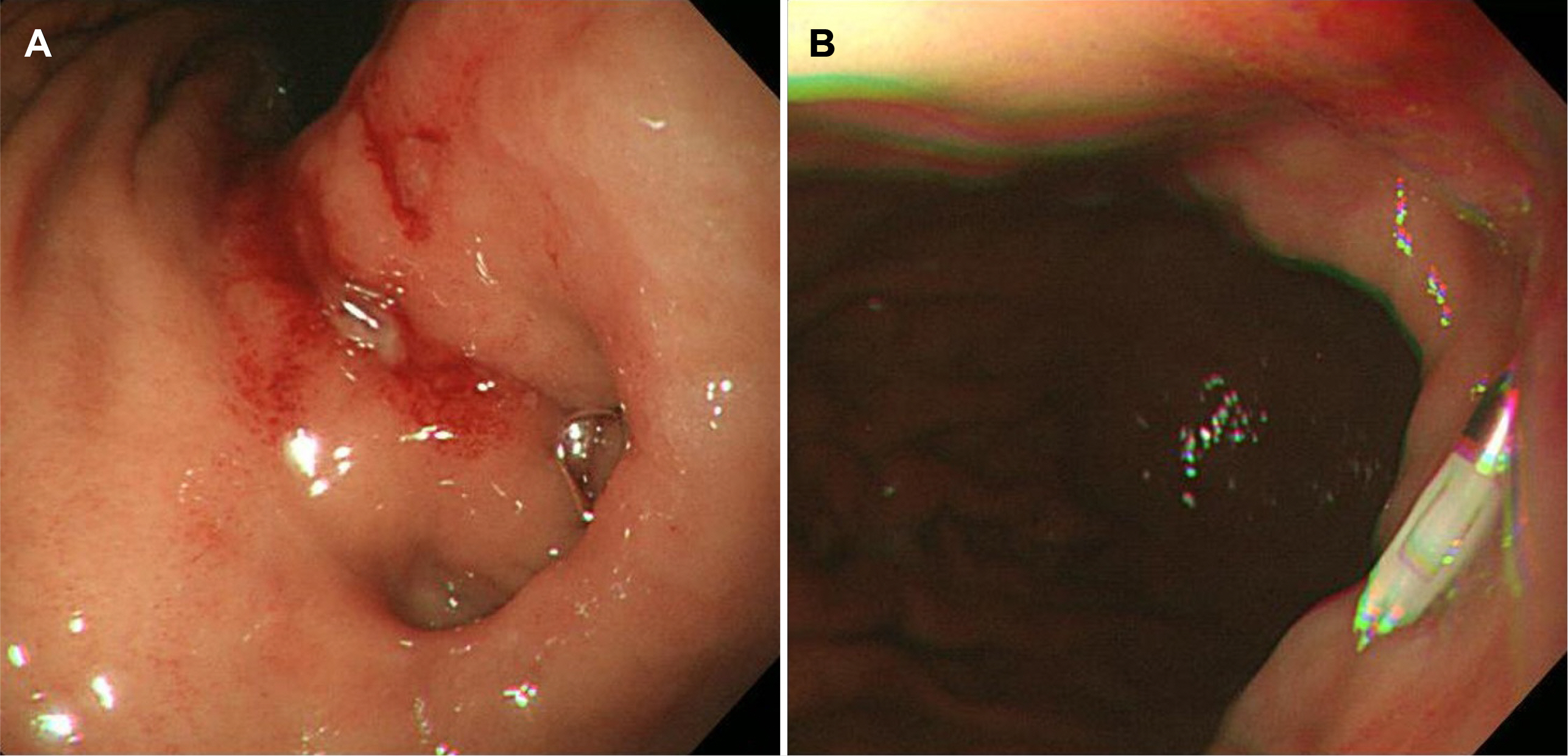
Fig. 1 Endoscopic finding. (A) J-turn view. A gastric ulcer in the posterior wall of the upper body and an opening leading to the duodenum. (B) Endoscopic hemostasis was performed with hemoclips.
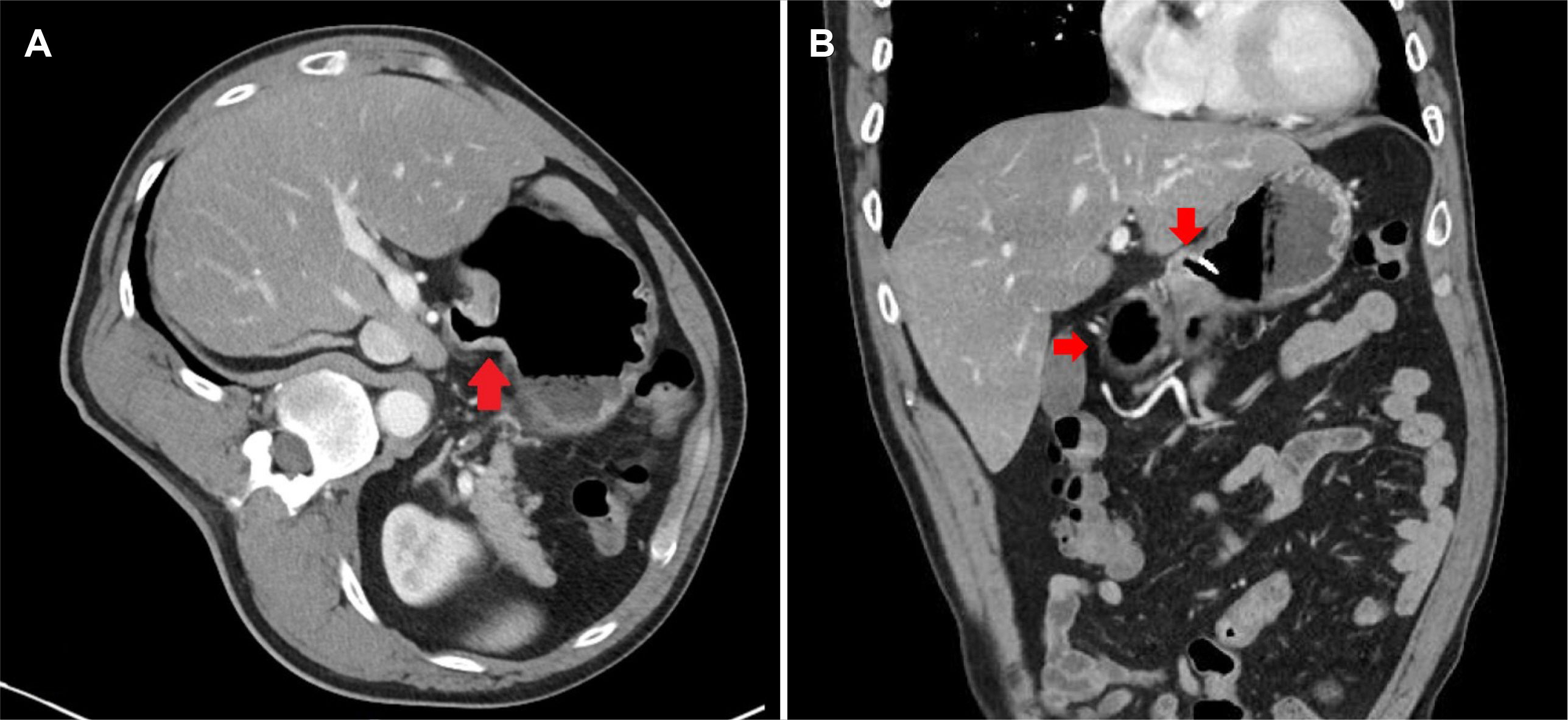
Fig. 2 Abdominal computed tomography scan. (A) Transverse view; the pylorus opened to the side of the posterior wall of the stomach (arrow). (B) Coronal view; a hemoclip is observed near the ectopic pyloric opening in the upper body, and the distal antrum is observed as a blind duct (arrows).

Fig. 3 Schematic figure of the stomach. (A) Normal stomach structure. (B) Gastric ectopic pyloric opening with gastric ulcer.
Reference
-
1. Ladd WE, Ware PF, Pickett LK. 1946; Congenital hypertrophic pyloric stenosis. J Am Med Assoc. 131:647–651. DOI: 10.1001/jama.1946.02870250001001. PMID: 20984883.
Article2. Einhorn RI, Grace ND, Banks PA. 1984; The clinical significance and natural history of the double pylorus. Dig Dis Sci. 29:213–218. DOI: 10.1007/BF01296254. PMID: 6697860.
Article3. Burdan F, Zinkiewicz K, Szumiło J, et al. 2012; Anatomical classification of the shape and topography of the operated stomach. Folia Morphol (Warsz). 71:129–135. PMID: 22936546.4. Burdan F, Rozylo-Kalinowska I, Szumilo J, et al. 2012; Anatomical classification of the shape and topography of the stomach. Surg Radiol Anat. 34:171–178. DOI: 10.1007/s00276-011-0893-8. PMID: 22057798. PMCID: PMC3284679.
Article5. Naidoo R, Singh B. 2012; Congenital double pylorus. Case Rep Gastrointest Med. 2012:537697. DOI: 10.1155/2012/537697. PMID: 22924137. PMCID: PMC3423775.
Article6. Teele RL, Smith EH. 1977; Ultrasound in the diagnosis of idiopathic hypertrophic pyloric stenosis. N Engl J Med. 296:1149–1150. DOI: 10.1056/NEJM197705192962006. PMID: 854046.
Article7. Lu B, Yang L. 2019; Gastric ectopic pyloric opening: an unusual case. Surg Radiol Anat. 41:1395–1398. DOI: 10.1007/s00276-019-02276-x. PMID: 31264000. PMCID: PMC6841747.
Article8. Chang CS, Chen GH, Kao CH, Wang SJ, Peng SN, Huang CK. 1996; The effect of Helicobacter pylori infection on gastric emptying of digestible and indigestible solids in patients with nonulcer dyspepsia. Am J Gastroenterol. 91:474–479. PMID: 8633494.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Pyloric Obstruction Due to Gastric Tuberculosis
- A Case of Neonatal Gastric Ulcer with Large Hematoma Presenting as Gastric Outlet Obstruction
- Three Cases of Coexistence of Gastric Cancer and Duodenal Ulcer
- Cytomegalovirus Gastric Ulcer Complicated with Pyloric Obstruction in a Patient with Ulcerative Colitis
- A Case of Double Pylorus Developed on the Gastric Body
