Korean J Pediatr Gastroenterol Nutr.
2011 Dec;14(4):398-402. 10.5223/kjpgn.2011.14.4.398.
A Case of Neonatal Gastric Ulcer with Large Hematoma Presenting as Gastric Outlet Obstruction
- Affiliations
-
- 1Department of Pediatrics, Hallym University Sacred Heart Hospital, Hallym University College of Medicine, Anyang, Korea. baby4019@hallym.or.kr
- 2Department of Diagnostic Radiology, Hallym University Sacred Heart Hospital, Hallym University College of Medicine, Anyang, Korea.
- KMID: 2277712
- DOI: http://doi.org/10.5223/kjpgn.2011.14.4.398
Abstract
- Gastric outlet obstruction (GOO) results from obstructing lesions in the region of the pyloric channel. In neonates, hypertrophic pyloric stenosis (HPS) is the most common cause while peptic ulcer is a rare cause. Neonatal gastric ulcer is relatively frequent in preterm newborn babies or in neonates treated in intensive care units. In healthy neonates, mucosal ulcers are associated with stressful conditions. In gastric ulcer diseases, gastric outlet obstruction is usually caused by a combination of edema, spasm, fibrotic stenosis and gastric atony. We experienced a case of neonatal gastric ulcer with a large hematoma in a 3-day-old infant presenting with repeated vomiting, poor oral intake, and abdominal distension. For the differential diagnosis, we did abdominal ultrasonography. Hematoma was diagnosed by abdominal ultrasonography. Endoscopic examination confirmed the hematoma and the presence of gastric ulcerations. We report this case with a brief review of the literature.
Keyword
MeSH Terms
Figure
-
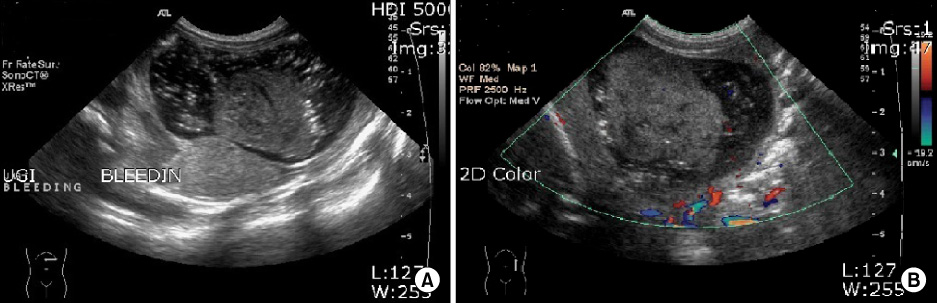
Fig. 1 (A) Ultrasonography shows a 3.3 cm sized round soft tissue echoic lesion suggestive of hematoma in the lumen of the stomach. (B) On color ultrasonography, no color flows are seen in the soft tissue lesion.
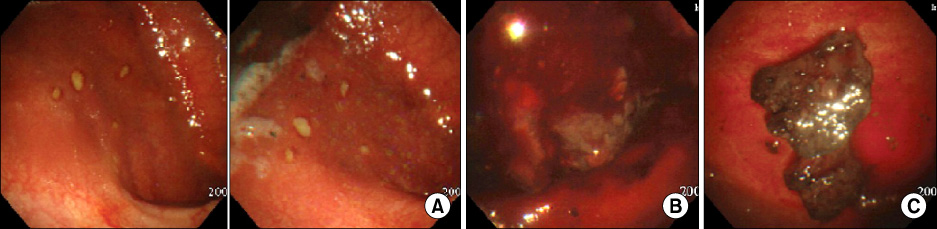
Fig. 2 (A) Multiple ulcers with an erythematous rim are seen in the stomach body. (B) A large hematoma is seen in the stomach fundus, before suction. (C) A hematoma is seen in the stomach fundus, after suction.
Reference
-
1. Feng J, Gu W, Li M, Yuan J, Weng Y, Wei M, et al. Rare causes of gastric outlet obstruction in children. Pediatr Surg Int. 2005. 21:635–640.
Article2. Azevedo S, Lopes J, Marques A, Mourato P, Freitas L, Lopes Al. Successful endoscopic resolution of a large gastric bezoar in a child. World J Gastrointest Endosc. 2011. 3:129–132.
Article3. Vallabhaneni P, Mansour M, Hutton K, Banerjee S. Lactobezoar-not so bizarre! Arch Dis Child Fetal Neonatal Ed. 2011. 96:F127.4. Hall NJ, Ward HC. Lactobezoar with perforation in a premature infant. Biol Neonate. 2005. 88:328–330.
Article5. Farin P, Janatuinen E. Sonographic detection of intragastric blood clot. Eur Radiol. 1997. 7:262–263.
Article6. Yen JB, Kong MS. Gastric outlet obstruction in pediatric patients. Chang Gung Med J. 2006. 29:401–405.7. Sharma KK, Agrawal P, Toshniwal H. Acquired gastric outlet obstruction during infancy and childhood; a report of five unusual cases. J Pediatr Surg. 1997. 32:928–930.
Article8. Jung J, Moon KR. A case of an antral web with a gastric ulcer due to Ibuprofen. Korean J Pediatr Gastroenterol Nutr. 2010. 13:66–69.
Article9. Boyle JT. Gastrointestinal bleeding in infants and children. Pediatr Rev. 2008. 29:39–52.
Article10. Park YS, Chung WC, Lee KM, Lee BI, Chun JS, Chang UI, et al. Massive gastric ulcer bleeding in a healthy full term infant. Korean J Gastroenterol. 2006. 48:210–214.11. Olives JP. Neonatal gastrointestinal endoscopy. Front Gastrointest Res. 1989. 15:65–73.
Article12. Madan A, Lavine J, Heyman MB, Townsend SF. Acute hemorrhagic gastritis in the newborn infant. J Perinatol. 1992. 12:377–380.13. Liebman WM, Thaler MM, Buvanover Y. Endoscopic evaluation of upper gastrointestinal bleeding in the newborn. Am J Gastroenterol. 1978. 69:607–608.14. Lazzaroni M, Petrillo M, Tornaghi R, Massironi E, Sainaghi M, Principi N, et al. Upper GI bleeding in healthy full-term infants: a case-control study. Am J Gastroenterol. 2002. 97:89–94.
Article15. Lee JW, Kwon KA, Kim KJ, Chung IK, Back MJ, Min YS, et al. The clinical usefulness of esophagogastroduodenoscopy in neonates and infants. Korean J Gastrointest Endosc. 2000. 20:425–430.16. Shin WJ, Shin JW, Ahn YH, Hwang JB, Han CH, Jung HL, et al. A Clinical evaluation of the esophagogastroduodenoscopy studies in Infants and early children. J Korean Pediatr Soc. 1996. 39:1280–1287.17. Caulfield M, Wyllie R, Sivak MV Jr, Michener W, Steffen R. Upper gastrointestinal tract endoscopy in the pediatric patient. J Pediatr. 1989. 115:339–345.
Article18. Fontana M, Tornaghi R, Petrillo M, Lora E, Bianchi PG, Principi N. Ranitidine treatment in newborn infants: effects on gastric acidity and serum prolactin levels. J Pediatr Gastroenterol Nutr. 1993. 16:406–411.19. Sarna MS, Saili A, Dutta AK, Sharma D. Stress associated gastric bleeding in newborn-role of ranitidine. Indian Pediatr. 1991. 28:1305–1308.20. Kelly DA. Do H2 receptor antagonists have a therapeutic role in childhood? J Pediatr Gastroenterol Nutr. 1994. 19:270–276.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Successful Endoscopic Decompression for Intramural Duodenal Hematoma with Gastric Outlet Obstruction Complicating Acute Pancreatitis
- A Case of Congenital Gastric Outlet Obstruction with Serosal Fibrous Band in Prematurity
- Three Cases of Gastric Polyps Producing Intermittent Gastric Outlet Obstruction
- A Case of Gastric Outlet Obstruction Complicated by Peptic Ulcer Secondary to Non-Steroidal Anti-Inflammatory Drug (NSAID)
- A Man with Dysphagia after Cervical Esophagogastrostomy: A Case Report
