J Korean Neurosurg Soc.
2022 Jan;65(1):22-29. 10.3340/jkns.2021.0064.
Outcomes of Mechanical Thrombectomy in Patients with Large Diffusion-Weighted Imaging Lesions
- Affiliations
-
- 1Busan Regional Cerebrovascular Center, Dong-A University Hospital, Busan, Korea
- 2Department of Neurosurgery, Dong-A University Hospital, Dong-A University College of Medicine, Busan, Korea
- KMID: 2523910
- DOI: http://doi.org/10.3340/jkns.2021.0064
Abstract
Objective
: Despite many advancements in endovascular treatment, the benefits of mechanical thrombectomy (MT) in patients with large infarctions remain uncertain due to hemorrhagic complications. Therefore, we aimed to investigate the efficacy and safety of recanalization via MT within 6 hours after stroke in patients with large cerebral infarction volumes (>70 mL).
Methods
: We retrospectively reviewed the medical data of 30 patients with large lesions on initial diffusion-weighted imaging (>70 mL) who underwent MT at our institution within 6 hours after stroke onset. Baseline data, recanalization rate, and 3-month clinical outcomes were analyzed. Successful recanalization was defined as a modified treatment in cerebral ischemia score of 2b or 3.
Results
: The recanalization rate was 63.3%, and symptomatic intracerebral hemorrhage occurred in six patients (20%). The proportion of patients with modified Rankin Scale (mRS) scores of 0–3 was significantly higher in the recanalization group than in the non-recanalization group (47.4% vs. 9.1%, p=0.049). The mortality rate was higher in the non-recanalization group, this difference was not significant (15.8% vs. 36.4%, p=0.372). In the analysis of 3-month clinical outcomes, only successful recanalization was significantly associated with mRS scores of 0–3 (90% vs. 50%, p=0.049). The odds ratio of recanalization for favorable outcomes (mRS 0–3) was 9.00 (95% confidence interval, 0.95–84.90; p=0.055).
Conclusion
: Despite the risk of symptomatic intracerebral hemorrhage, successful recanalization via MT 6 hours after stroke may improve clinical outcomes in patients with large vessel occlusion.
Keyword
Figure
-
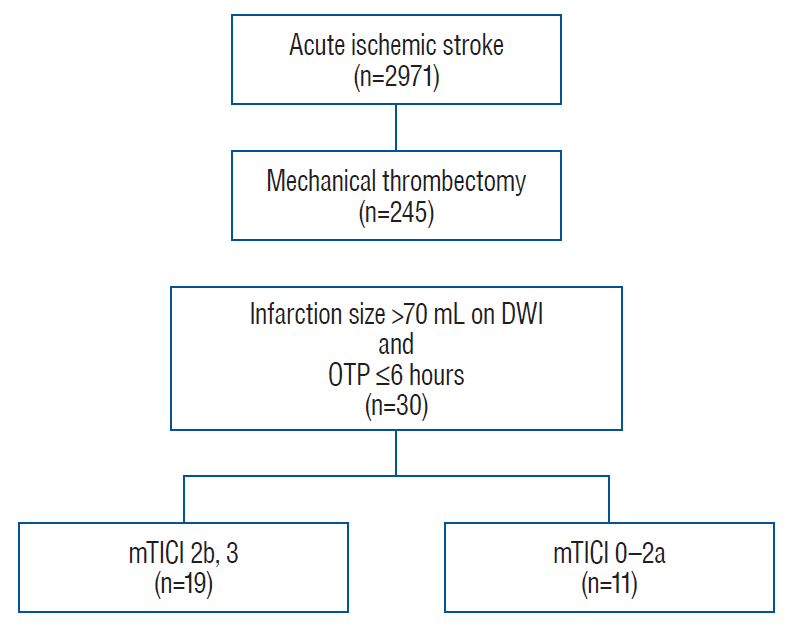
Fig. 1. Study flow chart. DWI : diffusion-weighted imaging, OTP : onset to puncture time, mTICI : modified Treatment in Cerebral Ischemia.
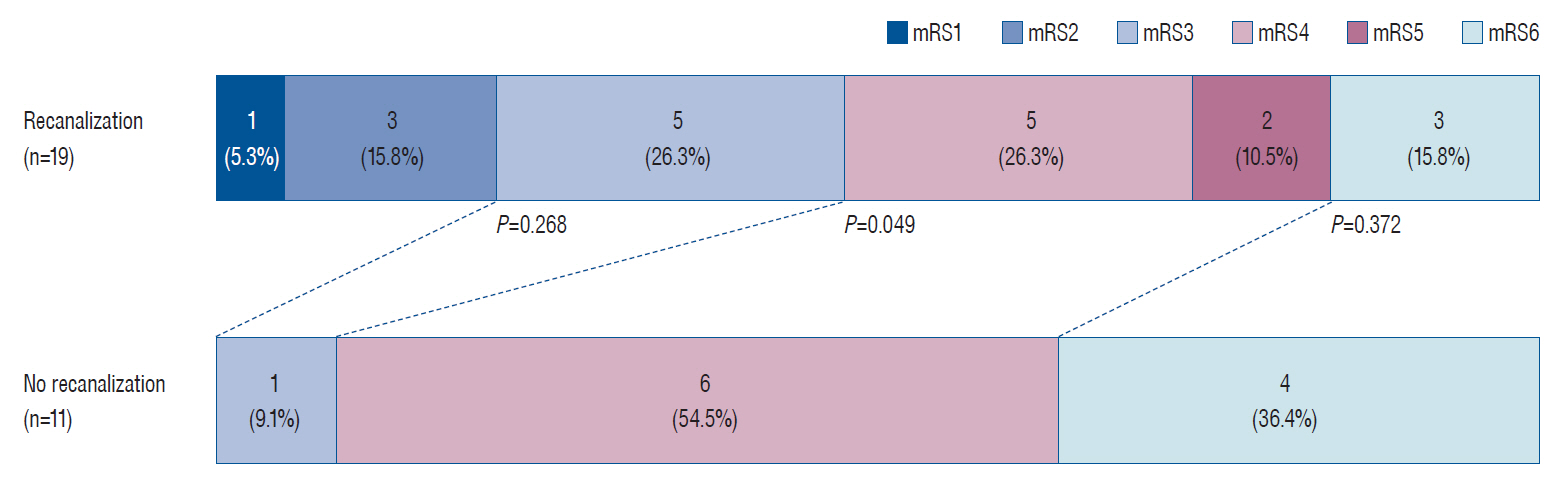
Fig. 2. Functional outcome at 3 months according to the recanalization status in patients with diffusion-weighted imaging lesions >70 mL. Although the proportion of patients with modified Rankin Scale (mRS) scores of 0–2 was higher in the recanalization group than in the non-recanalization group, this difference did not reach statistical significance (21.1% vs. 0%, p=0.268). However, the proportion of patients with mRS scores of 0–3 was also higher in the recanalization group (47.4% vs. 9.1%), and the difference was statistically significant (p=0.049).
Reference
-
References
1. Albers GW, Marks MP, Kemp S, Christensen S, Tsai JP, Ortega-Gutierrez S, et al. Thrombectomy for stroke at 6 to 16 hours with selection by perfusion imaging. N Engl J Med. 378:708–718. 2018.
Article2. Campbell BC, Purushotham A, Christensen S, Desmond PM, Nagakane Y, Parsons MW, et al. The infarct core is well represented by the acute diffusion lesion: sustained reversal is infrequent. J Cereb Blood Flow Metab. 32:50–56. 2012.
Article3. Gilgen MD, Klimek D, Liesirova KT, Meisterernst J, Klinger-Gratz PP, Schroth G, et al. Younger stroke patients with large pretreatment diffusion-weighted imaging lesions may benefit from endovascular treatment. Stroke. 46:2510–2516. 2015.
Article4. Goyal M, Menon BK, van Zwam WH, Dippel DW, Mitchell PJ, Demchuk AM, et al. Endovascular thrombectomy after large-vessel ischaemic stroke: a meta-analysis of individual patient data from five randomised trials. Lancet. 387:1723–1731. 2016.
Article5. Hao Y, Yang D, Wang H, Zi W, Zhang M, Geng Y, et al. Predictors for symptomatic intracranial hemorrhage after endovascular treatment of acute ischemic stroke. Stroke. 48:1203–1209. 2017.
Article6. Jovin TG, Yonas H, Gebel JM, Kanal E, Chang YF, Grahovac SZ, et al. The cortical ischemic core and not the consistently present penumbra is a determinant of clinical outcome in acute middle cerebral artery occlusion. Stroke. 34:2426–2433. 2003.
Article7. Kakita H, Yoshimura S, Uchida K, Sakai N, Yamagami H, Morimoto T, et al. Impact of endovascular therapy in patients with large ischemic core: subanalysis of recovery by endovascular salvage for cerebral ultra-acute embolism japan registry 2. Stroke. 50:901–908. 2019.8. Kerleroux B, Janot K, Dargazanli C, Daly-Eraya D, Ben-Hassen W, Zhu F, et al. Perfusion imaging to select patients with large ischemic core for mechanical thrombectomy. J Stroke. 22:225–233. 2020.
Article9. Kimura K, Iguchi Y, Shibazaki K, Terasawa Y, Inoue T, Uemura J, et al. Large ischemic lesions on diffusion-weighted imaging done before intravenous tissue plasminogen activator thrombolysis predicts a poor outcome in patients with acute stroke. Stroke. 39:2388–2391. 2008.
Article10. Nah HW, Kim DH, Kang M, Choi JH, Park HS, Cha JK. Thrombolysis in large diffusion-weighted imaging lesions: lower chance but still a chance. J Stroke Cerebrovasc Dis. 27:1511–1516. 2018.
Article11. National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. Tissue plasminogen activator for acute ischemic stroke. N Engl J Med. 333:1581–1587. 1995.12. Nawabi J, Kniep H, Schön G, Flottmann F, Leischner H, Kabiri R, et al. Hemorrhage after endovascular recanalization in acute stroke: lesion extent, collaterals and degree of ischemic water uptake mediate tissue vulnerability. Front Neurol. 10:569. 2019.
Article13. Nogueira RG, Jadhav AP, Haussen DC, Bonafe A, Budzik RF, Bhuva P, et al. Thrombectomy 6 to 24 hours after stroke with a mismatch between deficit and infarct. N Engl J Med. 378:11–21. 2018.14. Panni P, Gory B, Xie Y, Consoli A, Desilles JP, Mazighi M, et al. Acute stroke with large ischemic core treated by thrombectomy. Stroke. 50:1164–1171. 2019.15. Penumbra Pivotal Stroke Trial Investigators. The penumbra pivotal stroke trial: safety and effectiveness of a new generation of mechanical devices for clot removal in intracranial large vessel occlusive disease. Stroke. 40:2761–2768. 2009.16. Rangaraju S, Haussen D, Nogueira RG, Nahab F, Frankel M. Comparison of 3-month stroke disability and quality of life across modified rankin scale categories. Interv Neurol. 6:36–41. 2017.
Article17. Sawyer RN. Intravenous tissue plasminogen activator for large vessel ischemic stroke - is there still a role? Neurosurgery. 85(suppl_1):S34–S37. 2019.
Article18. Smith WS, Lev MH, English JD, Camargo EC, Chou M, Johnston SC, et al. Significance of large vessel intracranial occlusion causing acute ischemic stroke and TIA. Stroke. 40:3834–3840. 2009.
Article19. Smith WS, Sung G, Starkman S, Saver JL, Kidwell CS, Gobin YP, et al. Safety and efficacy of mechanical embolectomy in acute ischemic stroke: results of the MERCI trial. Stroke. 36:1432–1438. 2005.
Article20. Smith WS, Tsao JW, Billings ME, Johnston SC, Hemphill JC 3rd, Bonovich DC, et al. Prognostic significance of angiographically confirmed large vessel intracranial occlusion in patients presenting with acute brain ischemia. Neurocrit Care. 4:14–17. 2006.
Article21. Yoo AJ, Verduzco LA, Schaefer PW, Hirsch JA, Rabinov JD, González RG. MRI-based selection for intra-arterial stroke therapy: value of pretreatment diffusion-weighted imaging lesion volume in selecting patients with acute stroke who will benefit from early recanalization. Stroke. 40:2046–2054. 2009.
Article22. Zaidat OO, Yoo AJ, Khatri P, Tomsick TA, von Kummer R, Saver JL, et al. Recommendations on angiographic revascularization grading standards for acute ischemic stroke: a consensus statement. Stroke. 44:2650–2663. 2013.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Reversal of a Large Ischemic Lesion with Low Apparent Diffusion Coefficient Value by Rapid Spontaneous Recanalization
- Paradigm Shift in Intra-Arterial Mechanical Thrombectomy for Acute Ischemic Stroke : A Review of Randomized Controlled Trials after 2015
- The Brainstem Score on Diffusion-weighted Imaging before Mechanical Thrombectomy in Acute Basilar Artery Occlusion is a Reliable Predictor for Prognosis: A Comparative Study with Critical Area Perfusion Score on Perfusion MRI
- A Comparison of Lesion Detection and Conspicuity on T2-weighted Images (T2 FFE), FLAIR and Diffusion-weighted Images in Patients with Traumatic Brain Injury
- Diffusion-weighted MR Imaging after Intracranial Tumor Resection
