Prevention of Septal Perforation Using a Combination of Crushed Cartilage and Thin Silastic Sheet During Septoplasty
- Affiliations
-
- 1Department of Otolaryngology-Head and Neck Surgery, Dong-A University, College of Medicine, Busan, Republic of Korea
- KMID: 2522785
- DOI: http://doi.org/10.18787/jr.2021.00378
Abstract
- Background and Objectives
The aim of the present study was to investigate the effects of a combination of crushed cartilage and thin silastic sheet for patients with a risk of septal perforation during septoplasty.
Materials and Methods
A total of 195 people who underwent septoplasty surgery at Dong-A University Hospital from January 2019 to December 2020 were enrolled retrospectively. Among 195 people, our surgical method was provided for those with damage to both septal mucosa. The cartilage was collected, crushed with the cartilage crusher, and inserted between perforated mucosa. After the cartilage insertion, a 0.254-mm-thin silastic sheet was designed to cover both sides of the perforated septal mucosa. Next, a penetrating suture was placed. After thin silastic was applied on both mucosa, a 1-mm-thick silastic sheet was inserted on both sides of the nasal cavity and penetrating sutures were placed on the anterior and inferior septum. The operation concluded after packing both sides of the nasal cavity using non-absorbable packing material. The packing was removed on the second day after the operation, and the nasal cavity condition was checked every week. Thick silastic sheets were removed 5 days after surgery, and thin silastic sheets were maintained until both septal mucosa healed.
Results
Of nine total cases, only one 78-year-old male experienced septal perforation at the cartilage portion two months after surgery. In this case, no other action was taken to cover the perforation site because he reported no symptoms or discomfort during the 9 months after surgery. In the other eight cases, both septal mucosa healed completely, and there were no complications.
Conclusion
This method with crushed cartilage and silastic sheets to fill the defect after septal surgery is thought to help prevent postoperative perforation at no additional cost, and further research is needed.
Figure
-
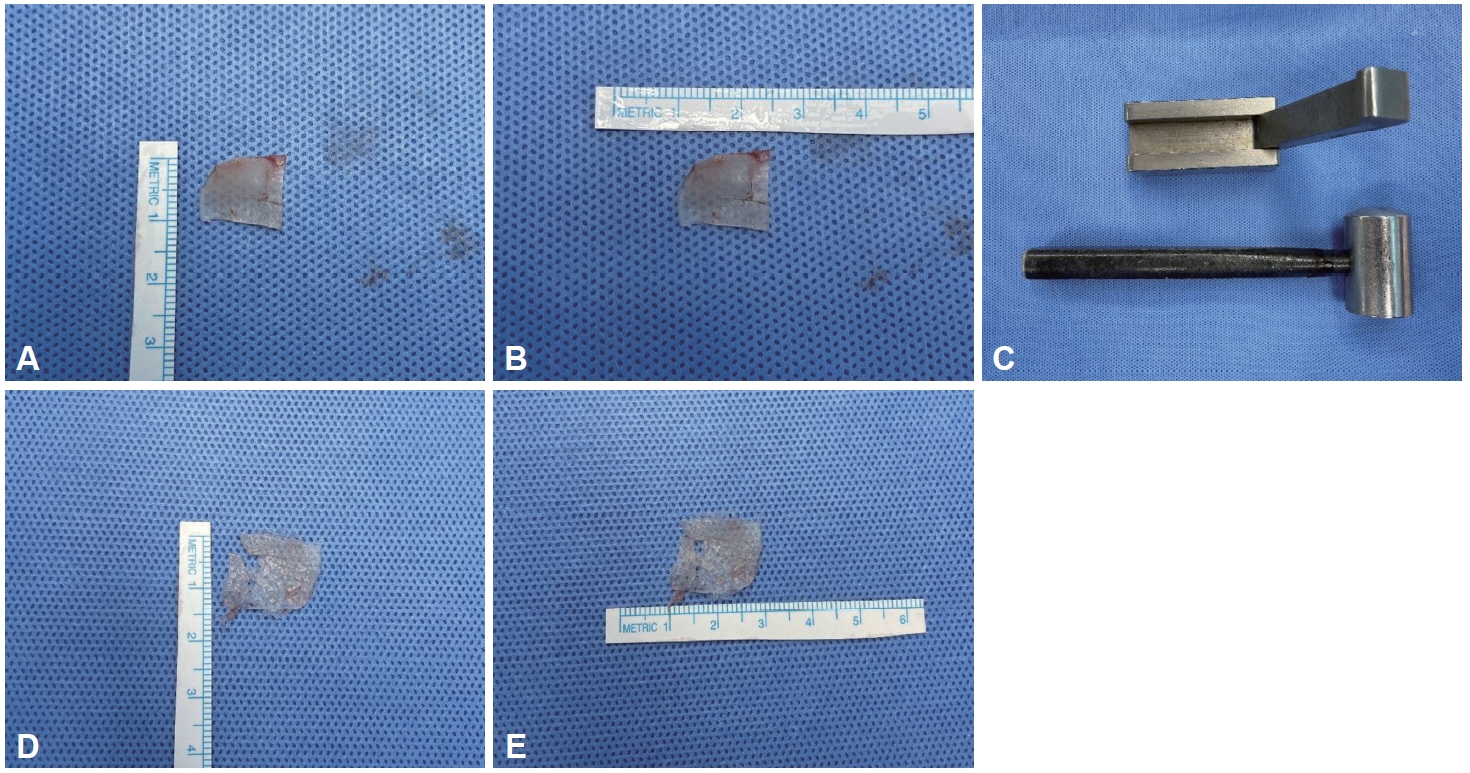
Fig. 1. Cartilage crusher and cartilage crushing. A: Autologous cartilage before crushing (length: 1 cm). B: Autologous cartilage before crushing (width: 1.5 cm). C: Cartilage crusher (Karl Storz Germany-5239; Karl Storz, Walsdorf, Germany). D: Autologous cartilage after crushing (length: 1.5 cm). E: Autologous cartilage after crushing (width: 2 cm).

Fig. 2. Intraoperative finding. A, B: Both septal mucosal was perforated. C: The crushed septal cartilage was inserted between the perforated mucosa. D, E: Thin silastic sheet (0.254 mm; Non-Reinforced Sheeting, Bioflexus, Kingman, AZ, USA) was covered on both perforated septal mucosa.
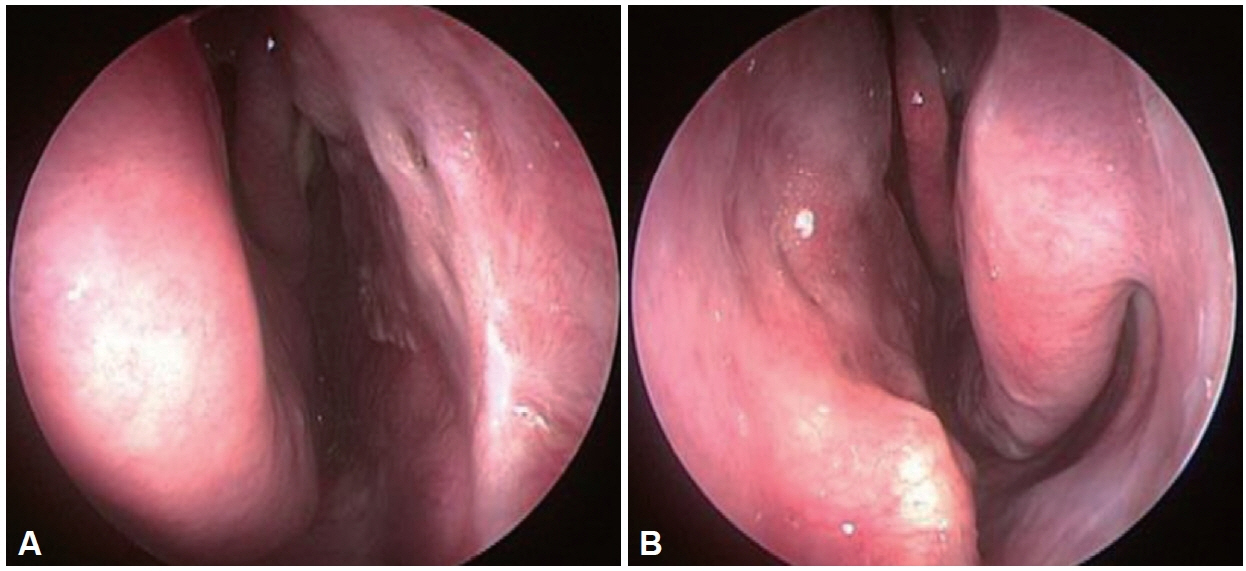
Fig. 3. Representative case where both septal mucosa well healed. A: Right nasal cavity. B: Left nasal cavity.

Fig. 4. Schematic diagram. S, septal cartilage; M, septal mucosa; CC, crushed cartilage; SS, silastic sheet (0.254 mm thickness; NonReinforced Sheeting, Bioflexus, Kingman, AZ, USA); TSS, thick silastic sheet (1 mm thickness; Internal Nasal Splint, MEDTRONIC, Minneapolis, MN, USA).
Reference
-
References
1. Quinn JG, Bonaparte JP, Kilty SJ. Postoperative management in the prevention of complications after septoplasty: a systematic review. Laryngoscope. 2013; 123(6):1328–33.2. Choi JS, Jin KH, Park MW, Kang SH, Lim DJ, Yu MS, et al. Prevention technique using inferior turbinate mucosal flap for septal perforation after septoplasty. J Rhinol. 2014; 21(1):37–40.3. Yun DH, Kim YJ, Kim JH, Lee BJ. Causes and clinical characteristics of the nasal septal perforation. J Rhinol. 2000; 7(1):64–8.4. Kridel RW. Septal perforation repair. Otolaryngol Clin North Am. 1999; 32(4):695–724.5. Lee JY, Lee SW, Lee JD, Lee YM, Shin JM, Lee JY. Usefulness of autologous cartilage and fibrin glue for the prevention of septal perforation during septal surgery: a preliminary report. Korean J Otolaryngol-Head Neck Surg. 2006; 49(6):611–5.6. Breadon GE, Kern EB, Neel HB 3rd. Autografts of uncrushed and crushed bone and cartilage. Experimental observations and clinical implications. Arch Otolaryngol. 1979; 105(2):75–80.7. Nolst Trenité GJ, Verwoerd CD, Verwoerd-Verhoef HL. Reimplantation of autologous septal cartilage in the growing nasal septum. II. The influence of reimplantation of rotated or crushed autologous septal cartilage on nasal growth: an experimental study in growing rabbits. Rhinology. 1988; 26(1):25–32.8. Cakmak O, Bircan S, Buyuklu F, Tuncer I, Dal T, Ozluoglu LN. Viability of crushed and diced cartilage grafts: a study in rabbits. Arch Facial Plast Surg. 2005; 7(1):21–6.9. Stoksted P, Ladefoged C. Crushed cartilage in nasal reconstruction. J Laryngol Otol. 1986; 100(8):897–906.10. Mutlu V. A novel surgical technique: crushed septal cartilage graft application in endonasal septoplasty. Auris Nasus Larynx. 2019; 46(2):218–22.11. Tanabe M, Takahashi H, Honjo I, Hasebe S, Sudo M. Factors affecting recovery of mastoid aeration after ear surgery. Eur Arch Otorhinolaryngol. 1999; 256(5):220–3.12. Hwang K, Kita Y. Alloplastic template fixation of blow-out fracture. J Craniofac Surg. 2002; 13(4):510–2.13. Schmidt BL, Lee C, Young DM, O’Brien J. Intraorbital squamous epithelial cyst: an unusual complication of Silastic implantation. J Craniofac Surg. 1998; 9(5):452–5. discussion 456-8.14. Alaani A, Jassar P, Smith I. The use of silastic nasal splints in the treatment of chronic epistaxis and nasal septal ulceration. Ear Nose Throat J. 2006; 85(11):738–9.15. Lee HR, Ahn DB, Park JH, Kim YH, Sin CM, Youn SJ, et al. Endoscopic repairment of septal perforation with using a unilateral nasal mucosal flap. Clin Exp Otorhinolaryngol. 2008; 1(3):154–7.16. Jung YG, Hong JW, Eun YG, Kim MG. Objective usefulness of thin silastic septal splints after septal surgery. Am J Rhinol Allergy. 2011; 25(3):182–5.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Prevention of Septal Perforation Using a Combination of Crushed Cartilage and Thin Silastic Sheet During Septoplasty
- Frequency of Nasal Septal Perforation at the Suture Fixation Site of a Silastic Sheet Inserted during Nasal Surgery
- A Securing Suture Technique of Autologous Cartilage for the Prevention of Septal Perforation during Septal Surgery
- Repair of Nasal Septal Perforation Using Silastic Sheet
- Prevention Technique Using Inferior Turbinate Mucosal Flap for Septal Perforation after Septoplasty
