The Clinical Impact of Capmatinib in the Treatment of Advanced Non–Small Cell Lung Cancer with MET Exon 14 Skipping Mutation or Gene Amplification
- Affiliations
-
- 1Center for Clinical Trials, National Cancer Center, Goyang, Korea
- 2Department of Pathology, National Cancer Center, Goyang, Korea
- 3Center for Lung Cancer, National Cancer Center, Goyang, Korea
- 4Department of Radiology, National Cancer Center, Goyang, Korea
- KMID: 2521578
- DOI: http://doi.org/10.4143/crt.2020.1331
Abstract
- Purpose
Capmatinib, an oral MET kinase inhibitor, has demonstrated its efficacy against non–small cell lung cancer (NSCLC) with MET dysregulation. We investigated its clinical impact in advanced NSCLC with MET exon 14 skipping mutation (METex14) or gene amplification.
Materials and Methods
Patients who participated in the screening of a phase II study of capmatinib for advanced NSCLC were enrolled in this study. MET gene copy number (GCN), protein expression, and METex14 were analyzed and the patients’ clinical outcome were retrospectively reviewed.
Results
A total of 72 patients were included in this analysis (group A: GCN ≥ 10 or METex14, n=14; group B: others, n=58). Among them, 13 patients were treated with capmatinib (group A, n=8; group B, n=5), and the overall response rate was 50% for group A, and 0% for group B. In all patients, the median overall survival (OS) was 20.2 months (95% confidence interval [CI], 6.9 to not applicable [NA]) for group A, and 11.3 months (95% CI, 8.2 to 20.3) for group B (p=0.457). However, within group A, median OS was 21.5 months (95% CI, 20.8 to NA) for capmatinib-treated, and 7.5 months (95% CI, 3.2 to NA) for capmatinib-untreated patients (p=0.025). Among all capmatinib-untreated patients (n=59), group A showed a trend towards worse OS to group B (median OS, 7.5 months vs. 11.3 months; p=0.123).
Conclusion
Our data suggest that capmatinib is a new compelling treatment for NSCLC with MET GCN ≥ 10 or METex14 based on the improved survival within these patients.
Keyword
Figure
-
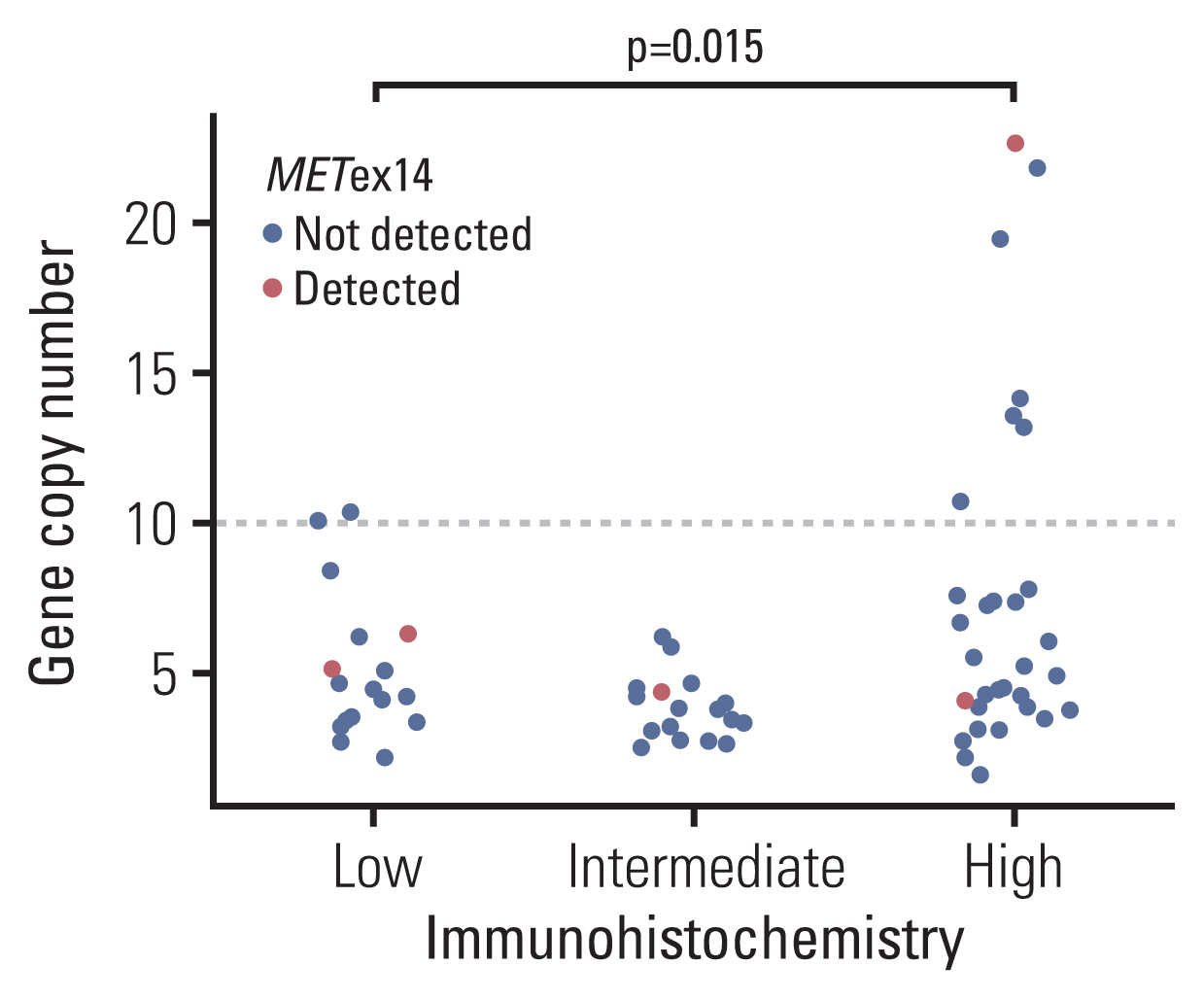
Fig. 1 Correlation of MET immunohistochemistry and gene copy numbers. Scatter plot of MET gene copy number values classified by immunohistochemistry staining results. A dotted line indicates the gene copy number threshold value of 10 copies per cell. Statistical analyses were performed using an ANOVA test. METex14, MET exon 14 skipping mutation.
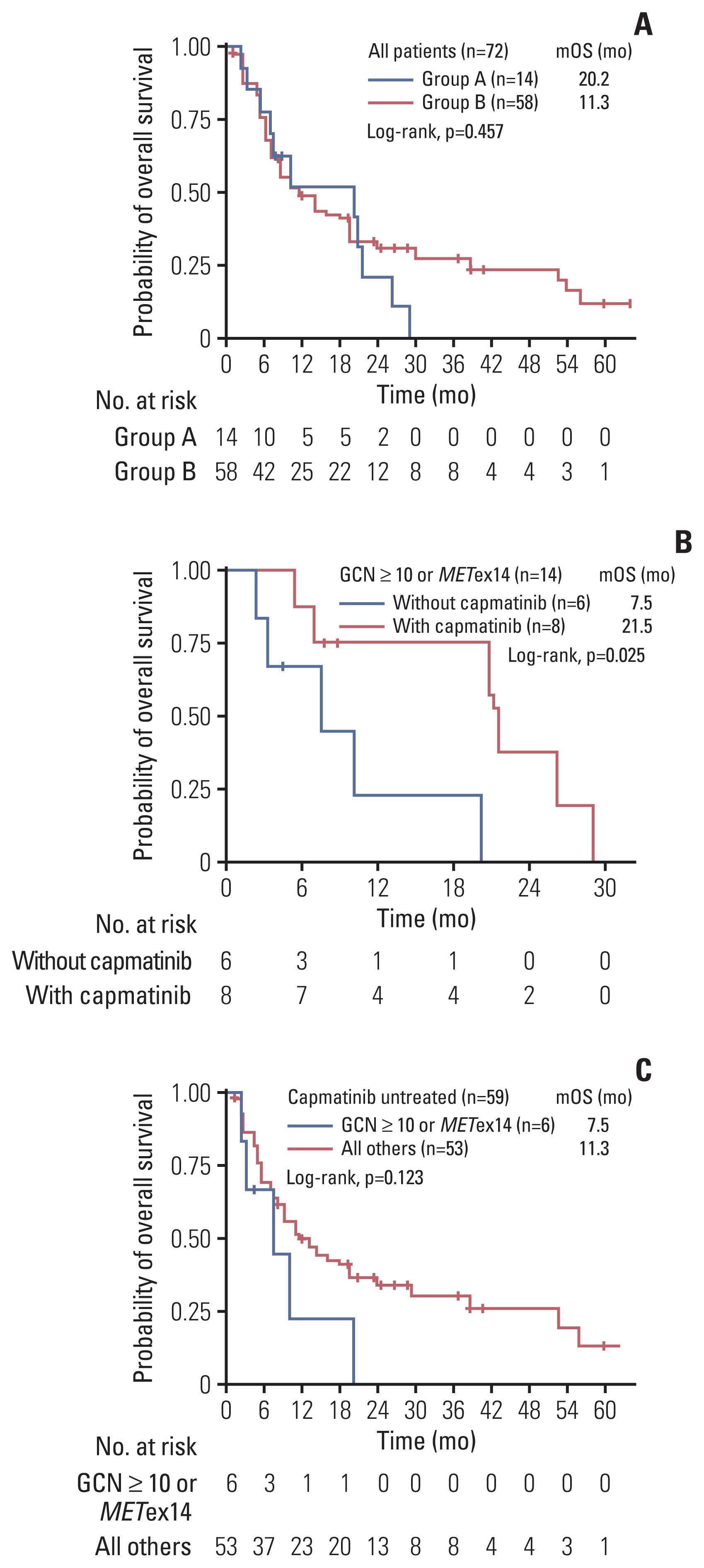
Fig. 2 Kaplan-Meier plots for overall survival. Kaplan-Meier plots for overall survival in all study patients (n=72) stratified by study groups (log-rank test, p=0.457) (A), patients with MET gene copy number (GCN) ≥ 10 or MET exon 14 skipping mutation (METex14) (n=14) stratified by capmatinib treatment (log-rank test, p=0.025) (B), and patients untreated with capmatinib (n=59) stratified by MET GCN levels (GCN > 10) and the presence of MET- ex14 (log-rank test, p=0.123) (C). mOS, median overall survival.
Reference
-
References
1. Ciuleanu T, Brodowicz T, Zielinski C, Kim JH, Krzakowski M, Laack E, et al. Maintenance pemetrexed plus best supportive care versus placebo plus best supportive care for non-small-cell lung cancer: a randomised, double-blind, phase 3 study. Lancet. 2009; 374:1432–40.
Article2. Scagliotti GV, Parikh P, von Pawel J, Biesma B, Vansteenkiste J, Manegold C, et al. Phase III study comparing cisplatin plus gemcitabine with cisplatin plus pemetrexed in chemotherapy-naive patients with advanced-stage non-small-cell lung cancer. J Clin Oncol. 2008; 26:3543–51.
Article3. Gandhi L, Rodriguez-Abreu D, Gadgeel S, Esteban E, Felip E, De Angelis F, et al. Pembrolizumab plus chemotherapy in metastatic non-small-cell lung cancer. N Engl J Med. 2018; 378:2078–92.
Article4. Gadgeel S, Rodriguez-Abreu D, Speranza G, Esteban E, Felip E, Domine M, et al. Updated analysis from KEYNOTE-189: pembrolizumab or placebo plus pemetrexed and platinum for previously untreated metastatic nonsquamous non-small-cell lung cancer. J Clin Oncol. 2020; 38:1505–17.
Article5. Ramalingam SS, Vansteenkiste J, Planchard D, Cho BC, Gray JE, Ohe Y, et al. Overall survival with osimertinib in untreated, EGFR-mutated advanced NSCLC. N Engl J Med. 2020; 382:41–50.
Article6. Peters S, Camidge DR, Shaw AT, Gadgeel S, Ahn JS, Kim DW, et al. Alectinib versus crizotinib in untreated ALK-positive non-small-cell lung cancer. N Engl J Med. 2017; 377:829–38.
Article7. Trusolino L, Bertotti A, Comoglio PM. MET signalling: principles and functions in development, organ regeneration and cancer. Nat Rev Mol Cell Biol. 2010; 11:834–48.
Article8. Liu X, Newton RC, Scherle PA. Developing c-MET pathway inhibitors for cancer therapy: progress and challenges. Trends Mol Med. 2010; 16:37–45.
Article9. Salgia R. MET in lung cancer: biomarker selection based on scientific rationale. Mol Cancer Ther. 2017; 16:555–65.
Article10. Tong JH, Yeung SF, Chan AW, Chung LY, Chau SL, Lung RW, et al. MET amplification and exon 14 splice site mutation define unique molecular subgroups of non-small cell lung carcinoma with poor prognosis. Clin Cancer Res. 2016; 22:3048–56.
Article11. Cappuzzo F, Marchetti A, Skokan M, Rossi E, Gajapathy S, Felicioni L, et al. Increased MET gene copy number negatively affects survival of surgically resected non-small-cell lung cancer patients. J Clin Oncol. 2009; 27:1667–74.12. Frampton GM, Ali SM, Rosenzweig M, Chmielecki J, Lu X, Bauer TM, et al. Activation of MET via diverse exon 14 splicing alterations occurs in multiple tumor types and confers clinical sensitivity to MET inhibitors. Cancer Discov. 2015; 5:850–9.
Article13. Paik PK, Drilon A, Fan PD, Yu H, Rekhtman N, Ginsberg MS, et al. Response to MET inhibitors in patients with stage IV lung adenocarcinomas harboring MET mutations causing exon 14 skipping. Cancer Discov. 2015; 5:842–9.
Article14. Go H, Jeon YK, Park HJ, Sung SW, Seo JW, Chung DH. High MET gene copy number leads to shorter survival in patients with non-small cell lung cancer. J Thorac Oncol. 2010; 5:305–13.
Article15. Ou SH, Kwak EL, Siwak-Tapp C, Dy J, Bergethon K, Clark JW, et al. Activity of crizotinib (PF02341066), a dual mesenchymal-epithelial transition (MET) and anaplastic lymphoma kinase (ALK) inhibitor, in a non-small cell lung cancer patient with de novo MET amplification. J Thorac Oncol. 2011; 6:942–6.
Article16. Schwab R, Petak I, Kollar M, Pinter F, Varkondi E, Kohanka A, et al. Major partial response to crizotinib, a dual MET/ALK inhibitor, in a squamous cell lung (SCC) carcinoma patient with de novo c-MET amplification in the absence of ALK rearrangement. Lung Cancer. 2014; 83:109–11.
Article17. Kong-Beltran M, Seshagiri S, Zha J, Zhu W, Bhawe K, Mendoza N, et al. Somatic mutations lead to an oncogenic deletion of met in lung cancer. Cancer Res. 2006; 66:283–9.
Article18. Ma PC, Jagadeeswaran R, Jagadeesh S, Tretiakova MS, Nallasura V, Fox EA, et al. Functional expression and mutations of c-Met and its therapeutic inhibition with SU11274 and small interfering RNA in non-small cell lung cancer. Cancer Res. 2005; 65:1479–88.
Article19. Jenkins RW, Oxnard GR, Elkin S, Sullivan EK, Carter JL, Barbie DA. Response to crizotinib in a patient with lung adenocarcinoma harboring a MET splice site mutation. Clin Lung Cancer. 2015; 16:e101–4.
Article20. Mendenhall MA, Goldman JW. MET-mutated NSCLC with major response to crizotinib. J Thorac Oncol. 2015; 10:e33–4.
Article21. Waqar SN, Morgensztern D, Sehn J. MET mutation associated with responsiveness to crizotinib. J Thorac Oncol. 2015; 10:e29–31.
Article22. Schrock AB, Frampton GM, Suh J, Chalmers ZR, Rosenzweig M, Erlich RL, et al. Characterization of 298 patients with lung cancer harboring MET exon 14 skipping alterations. J Thorac Oncol. 2016; 11:1493–502.
Article23. Drilon A, Clark JW, Weiss J, Ou SI, Camidge DR, Solomon BJ, et al. Antitumor activity of crizotinib in lung cancers harboring a MET exon 14 alteration. Nat Med. 2020; 26:47–51.
Article24. Schildhaus HU, Schultheis AM, Ruschoff J, Binot E, Merkelbach-Bruse S, Fassunke J, et al. MET amplification status in therapy-naive adeno- and squamous cell carcinomas of the lung. Clin Cancer Res. 2015; 21:907–15.25. Cancer Genome Atlas Research Network. Comprehensive molecular profiling of lung adenocarcinoma. Nature. 2014; 511:543–50.26. Awad MM, Oxnard GR, Jackman DM, Savukoski DO, Hall D, Shivdasani P, et al. MET exon 14 mutations in non-small-cell lung cancer are associated with advanced age and stage-dependent MET genomic amplification and c-Met overexpression. J Clin Oncol. 2016; 34:721–30.
Article27. Liu X, Wang Q, Yang G, Marando C, Koblish HK, Hall LM, et al. A novel kinase inhibitor, INCB28060, blocks c-MET-dependent signaling, neoplastic activities, and cross-talk with EGFR and HER-3. Clin Cancer Res. 2011; 17:7127–38.
Article28. Wolf J, Seto T, Han JY, Reguart N, Garon EB, Groen HJ, et al. Capmatinib in MET exon 14-mutated or MET-amplified non-small-cell lung cancer. N Engl J Med. 2020; 383:944–57.29. Watermann I, Schmitt B, Stellmacher F, Muller J, Gaber R, Kugler C, et al. Improved diagnostics targeting c-MET in non-small cell lung cancer: expression, amplification and activation? Diagn Pathol. 2015; 10:130.
Article30. Wang M, Liang L, Lei X, Multani A, Meric-Bernstam F, Tripathy D, et al. Evaluation of cMET aberration by immunohistochemistry and fluorescence in situ hybridization (FISH) in triple negative breast cancers. Ann Diagn Pathol. 2018; 35:69–76.
Article31. Finocchiaro G, Toschi L, Gianoncelli L, Baretti M, Santoro A. Prognostic and predictive value of MET deregulation in non-small cell lung cancer. Ann Transl Med. 2015; 3:83.32. Schuler M, Berardi R, Lim WT, de Jonge M, Bauer TM, Azaro A, et al. Molecular correlates of response to capmatinib in advanced non-small-cell lung cancer: clinical and biomarker results from a phase I trial. Ann Oncol. 2020; 31:789–97.
Article33. Park S, Koh J, Kim DW, Kim M, Keam B, Kim TM, et al. MET amplification, protein expression, and mutations in pulmonary adenocarcinoma. Lung Cancer. 2015; 90:381–7.
Article34. Liu X, Jia Y, Stoopler MB, Shen Y, Cheng H, Chen J, et al. Next-generation sequencing of pulmonary sarcomatoid carcinoma reveals high frequency of actionable MET gene mutations. J Clin Oncol. 2016; 34:794–802.
Article35. Schrock AB, Li SD, Frampton GM, Suh J, Braun E, Mehra R, et al. Pulmonary sarcomatoid carcinomas commonly harbor either potentially targetable genomic alterations or high tumor mutational burden as observed by comprehensive genomic profiling. J Thorac Oncol. 2017; 12:932–42.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Robust home brew fragment sizing assay for detection of MET exon 14 skipping mutation in non–small cell lung cancer patients in resource constrained community hospitals
- Prevalence and Clinicopathological Significance of METOverexpression and Gene Amplification in Patients withGallbladder Carcinoma
- Acquired Resistance of MET-Amplified Non-small Cell Lung Cancer Cells to the MET Inhibitor Capmatinib
- Analysis of TP53 Gene Mutations in the Korean Patients with Lung Cancer
- Evaluation of MET alteration in EGFR-mutant non-small cell lung cancer patients treated with EGFR tyrosine kinase inhibitor from paired biopsy: A retrospective cohort study
