Successful laparoscopic surgery of accessory cavitated uterine mass in young women with severe dysmenorrhea
- Affiliations
-
- 1Department of Obstetrics and Gynecology, Keimyung University School of Medicine, Daegu, Korea
- 2Department of Forensic Medicine, School of Medicine, Kyungpook National University, Daegu, Korea
- KMID: 2518666
- DOI: http://doi.org/10.12701/yujm.2020.00696
Abstract
- Accessory cavitated uterine mass (ACUM) is a rare and unique condition seen in young women. We report cases of ACUMs in two patients, a 14-year-old girl and a 25-year-old woman, both with complaints of severe dysmenorrhea that had started at menarche and had progressively worsened since. A large cystic lesion was localized in the anterolateral wall of the myometrium separate from the endometrium, which was difficult to distinguish from congenital uterine anomalies. Laparoscopic excision of the ACUMs was successful and completely resolved the dysmenorrhea. Early investigation of severe dysmenorrhea in young women can provide appropriate management and relieve symptoms.
Keyword
Figure
-
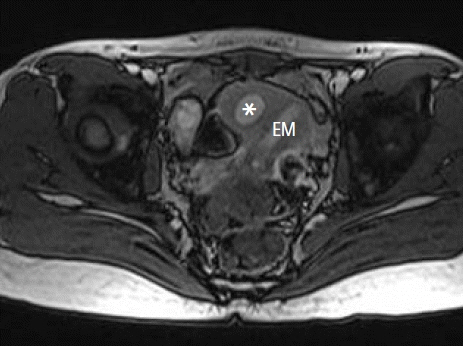
Fig. 1. Pelvic magnetic resonance imaging revealing a large cystic lesion (accessory cavitated uterine mass, asterisk) localized in the right side of the uterus, independent of the normal endometrium and ovaries. EM, endometrial cavity.
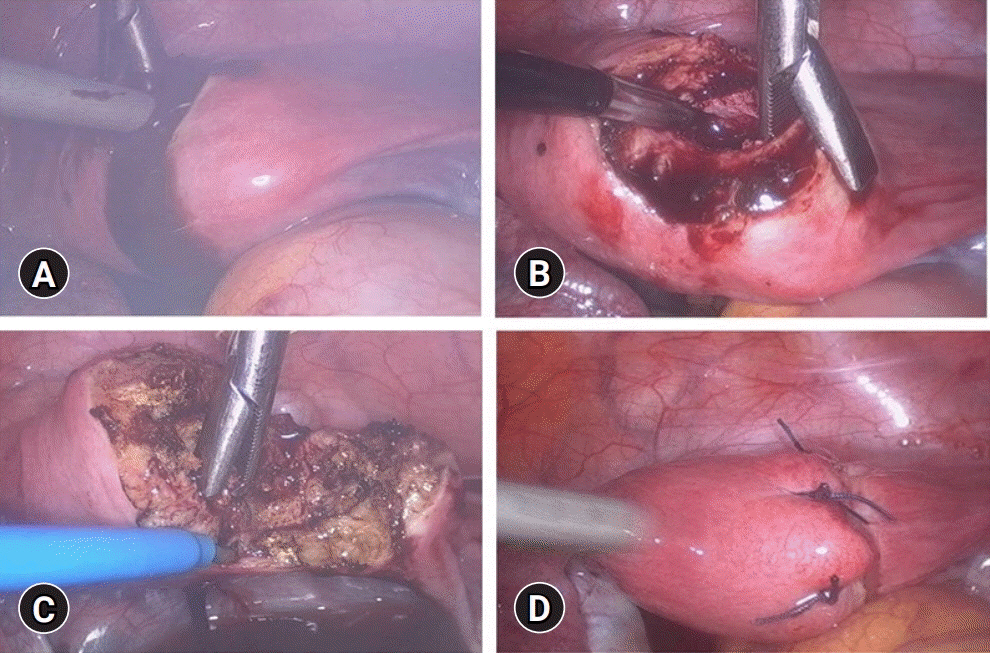
Fig. 2. Laparoscopic mass excision. (A) After incision, chocolate-like fluid was expressed from the cystic cavity. (B) Cystic cavity seen after irrigation. (C) The surrounding endometrial and myometrial tissue of the cyst completely resected using the monopolar hook. (D) Myometrial defect sutured for two to three layers.

Fig. 3. Histological section showing cyst wall lined with endometrial stromal cells, surrounded by myometrium (hematoxylin and eosin stain, ×200).

Fig. 4. Pelvic magnetic resonance imaging revealing a large cystic lesion (accessory cavitated uterine mass, asterisk) localized in the left side of the uterus, apart from the normal endometrium. Polycystic ovaries were also found. EM, endometrial cavity.
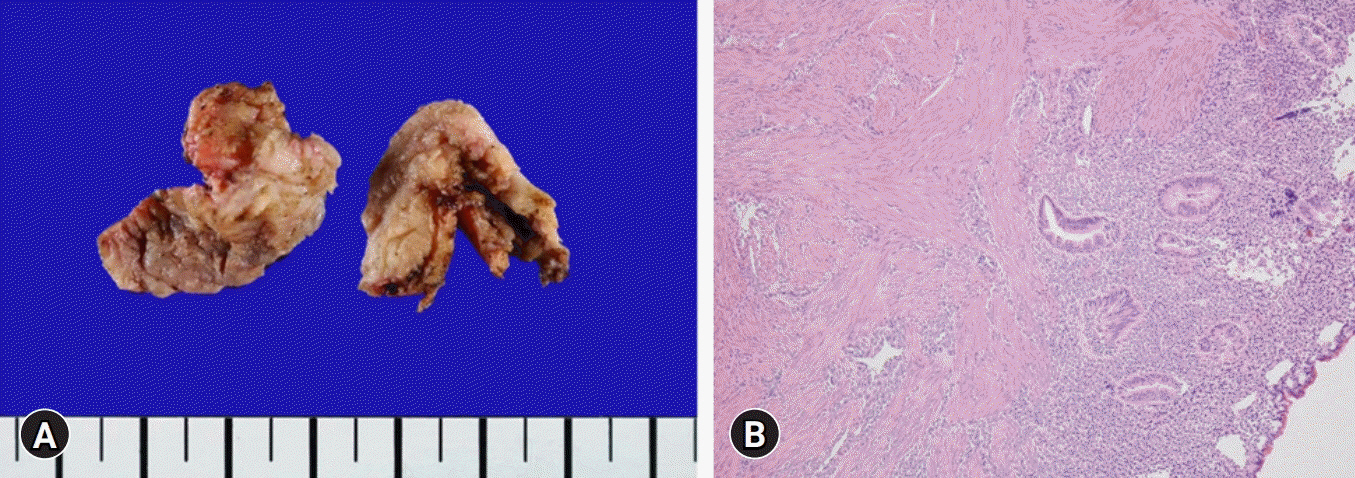
Fig. 5. (A) The excised specimens are irregularly shaped cystic structure with focal hemorrhage. (B) Histologic section showing the cyst wall lined with endometrial glandular epithelium and stromal cells, surrounded by myometrium. Adenomyotic lesions were not revealed in the surrounding myometrium (hematoxylin and eosin stain, ×100).
Reference
-
References
1. Bedaiwy MA, Henry DN, Elguero S, Pickett S, Greenfield M. Accessory and cavitated uterine mass with functional endometrium in an adolescent: diagnosis and laparoscopic excision technique. J Pediatr Adolesc Gynecol. 2013; 26:e89–91.
Article2. Tamai K, Koyama T, Umeoka S, Saga T, Fujii S, Togashi K. Spectrum of MR features in adenomyosis. Best Pract Res Clin Obstet Gynaecol. 2006; 20:583–602.
Article3. Nabeshima H, Murakami T, Nishimoto M, Sugawara N, Sato N. Successful total laparoscopic cystic adenomyomectomy after unsuccessful open surgery using transtrocar ultrasonographic guiding. J Minim Invasive Gynecol. 2008; 15:227–30.
Article4. Acién P, Acién M, Fernández F, José Mayol M, Aranda I. The cavitated accessory uterine mass: a Müllerian anomaly in women with an otherwise normal uterus. Obstet Gynecol. 2010; 116:1101–9.
Article5. Jain N, Verma R. Imaging diagnosis of accessory and cavitated uterine mass, a rare mullerian anomaly. Indian J Radiol Imaging. 2014; 24:178–81.
Article6. Paul PG, Chopade G, Das T, Dhivya N, Patil S, Thomas M. Accessory cavitated uterine mass: a rare cause of severe dysmenorrhea in young women. J Minim Invasive Gynecol. 2015; 22:1300–3.
Article7. Takeda A, Sakai K, Mitsui T, Nakamura H. Laparoscopic management of juvenile cystic adenomyoma of the uterus: report of two cases and review of the literature. J Minim Invasive Gynecol. 2007; 14:370–4.
Article8. Brosens I, Gordts S, Habiba M, Benagiano G. Uterine cystic adenomyosis: a disease of younger women. J Pediatr Adolesc Gynecol. 2015; 28:420–6.
Article9. Nabeshima H, Murakami T, Terada Y, Noda T, Yaegashi N, Okamura K. Total laparoscopic surgery of cystic adenomyoma under hydroultrasonographic monitoring. J Am Assoc Gynecol Laparosc. 2003; 10:195–9.
Article10. Takeuchi H, Kitade M, Kikuchi I, Kumakiri J, Kuroda K, Jinushi M. Diagnosis, laparoscopic management, and histopathologic findings of juvenile cystic adenomyoma: a review of nine cases. Fertil Steril. 2010; 94:862–8.
Article11. Fisseha S, Smith YR, Kumetz LM, Mueller GC, Hussain H, Quint EH. Cystic myometrial lesion in the uterus of an adolescent girl. Fertil Steril. 2006; 86:716–8.
Article12. Pontrelli G, Bounous VE, Scarperi S, Minelli L, Di Spiezio Sardo A, Florio P. Rare case of giant cystic adenomyoma mimicking a uterine malformation, diagnosed and treated by hysteroscopy. J Obstet Gynaecol Res. 2015; 41:1300–4.
Article13. Kim MJ. A case of cystic adenomyoma of the uterus after complete abortion without transcervical curettage. Obstet Gynecol Sci. 2014; 57:176–9.
Article14. Tahlan A, Nanda A, Mohan H. Uterine adenomyoma: a clinicopathologic review of 26 cases and a review of the literature. Int J Gynecol Pathol. 2006; 25:361–5.15. Ho ML, Ratts V, Merritt D. Adenomyotic cyst in an adolescent girl. J Pediatr Adolesc Gynecol. 2009; 22:e33–8.
Article16. Ryo E, Takeshita S, Shiba M, Ayabe T. Radiofrequency ablation for cystic adenomyosis: a case report. J Reprod Med. 2006; 51:427–30.17. Kumakiri J, Kikuchi I, Sogawa Y, Jinushi M, Aoki Y, Kitade M, et al. Single-incision laparoscopic surgery using an articulating monopolar for juvenile cystic adenomyoma. Minim Invasive Ther Allied Technol. 2013; 22:312–5.
Article18. Akar ME, Leezer KH, Yalcinkaya TM. Robot-assisted laparoscopic management of a case with juvenile cystic adenomyoma. Fertil Steril. 2010; 94:e55–6.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Laparoscopic excision of uterine horn in case of unicornuate uterus firmly attached with non-communicating rudimentary horn
- A Case of Intrauterine Pregnancy after Laparoscopic Bilateral Uterine Artery Ligation for Treatment Uterine Myoma
- Stellate Ganglion Block for the Treatment of Primary Dysmenorrhea
- Weight Changes and Unhealthy Weight Control Behaviors Are Associated With Dysmenorrhea in Young Women
- Comparison of Laparoscopic Radiofrequency Myolysis (LRFM) and Ultrasonographic Radiofrequency Myolysis (URFM) in Treatment of Midline Dysmenorrhea
