J Korean Neurosurg Soc.
2021 May;64(3):380-385. 10.3340/jkns.2021.0025.
Caudal Agenesis : Understanding the Base of the Wide Clinical Spectrum
- Affiliations
-
- 1Division of Pediatric Neurosurgery, Seoul National University Children’s Hospital, Seoul, Korea
- 2Department of Anatomy, Seoul National University College of Medicine, Seoul, Korea
- 3Neuro-oncology Clinic, Center for Rare Cancers, National Cancer Center, Goyang, Korea
- KMID: 2515494
- DOI: http://doi.org/10.3340/jkns.2021.0025
Abstract
- Caudal agenesis refers to the congenital malformation with the essential feature of the agenesis of the sacrococcygeal bone. It is associated with various types of spinal cord anomaly as well as with complex anomalies of genitourinary or gastrointestinal system. The wide spectrum of the disease can be attributed to its pathoembryological origin, the secondary neurulation. This review presents the definition, etiology, classification, and clinical features of the disease.
Keyword
Figure
-
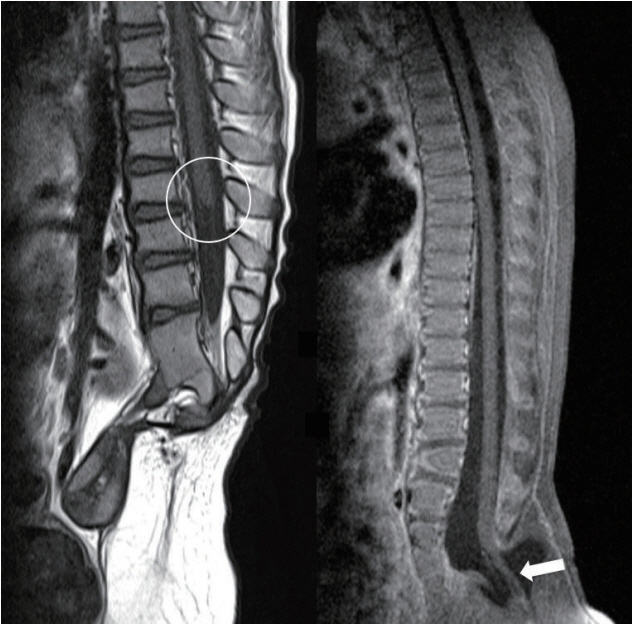
Fig. 1. Left : Failure of formation type of caudal agenesis shows the blunt ended conus (circle) usually at the location at or above L1. Right : Failure of regression type of caudal agenesis shows low-lying conus. This case shows the retained medullary cord with the conus below the upper sacral level (arrow).

Fig. 2. A schematic drawing summarizing a new classification system integrating the level of conus and the feature (shape and associated anomaly) of the spinal cord. This classification allows the designation of cases according to the pathoembryogenesis (failure of formation vs. failure of regression).
Reference
-
References
1. Andrish J, Kalamchi A, MacEwen GD. Sacral agenesis: a clinical evaluation of its management, heredity, and associated anomalies. Clin Orthop Relat Res. (139):52–57. 1979.2. Balioğlu MB, Akman YE, Ucpunar H, Albayrak A, Kargın D, Atıcı Y, et al. Sacral agenesis: evaluation of accompanying pathologies in 38 cases, with analysis of long-term outcomes. Childs Nerv Syst. 32:1693–1702. 2016.
Article3. Banta JV, Nichols O. Sacral agenesis. J Bone Joint Surg Am. 51:693–703. 1969.
Article4. Barkovich AJ, Raghavan N, Chuang S, Peck WW. The wedge-shaped cord terminus: a radiographic sign of caudal regression. AJNR Am J Neuroradiol. 10:1223–1231. 1989.5. Denton JR. The association of congenital spinal anomalies with imperforate anus. Clin Orthop Relat Res. (162):91–98. 1982.
Article6. Emami-Naeini P, Rahbar Z, Nejat F, Kajbafzadeh A, El Khashab M. Neurological presentations, imaging, and associated anomalies in 50 patients with sacral agenesis. Neurosurgery. 67:894–900. discussion900. 2010.
Article7. Guzman L, Bauer SB, Hallett M, Khoshbin S, Colodny AH, Retik AB. Evaluation and management of children with sacral agenesis. Urology. 22:506–510. 1983.
Article8. Lee JY, Pang D, Wang KC. Caudal Agenesis and Associated Spinal Cord Malformations. In : Rocco CD, Pang D, Rutka JT, editors. Textbook of Pediatric Neurosurgery. Cham: Springer International Publishing;2020. p. 2557–2575.9. Mills JL. Malformations in infants of diabetic mothers. Teratology. 25:385–394. 1982.
Article10. Müller F, O’Rahilly R. The development of the human brain, the closure of the caudal neuropore, and the beginning of secondary neurulation at stage 12. Anat Embryol (Berl). 176:413–430. 1987.
Article11. Nour S, Kumar D, Dickson JA. Anorectal malformations with sacral bony abnormalities. Arch Dis Child. 64:1618–1620. 1989.
Article12. Pang D. Sacral agenesis and caudal spinal cord malformations. Neurosurgery. 32:755–778. discussion 778-779. 1993.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Agenesis of Corpus Callosum
- Disorders of Secondary Neurulation : Mainly Focused on Pathoembryogenesis
- A Case of Acrocallosal Syndrome with Developmental Delay: A case report
- MRI Findings of Type II Sacral Agenesis: A Case Report and Literature Review
- Cerebellar Ectopia Associated with Unilateral Agenesis of Posterior Arch of Atlas
